
American Heart Association Training Center
Cardiac arrest during pregnancy is rare but life-threatening for both mother and fetus. Its causes often differ from those in the general population and include obstetric complications such as postpartum hemorrhage, amniotic fluid embolism, severe preeclampsia or eclampsia, and placental abruption, along with common reversible causes like hypovolemia, hypoxia, electrolyte imbalances, thrombosis, and toxins. Clinicians must recognize cardiac arrest immediately and act quickly, coordinating care among obstetric, anesthesia, and neonatal specialists. Resuscitation follows standard advanced cardiac life support principles, with important adjustments for pregnancy: left uterine displacement to relieve aortocaval compression, slightly higher hand placement for chest compressions, and early airway management.


The Cardiac Arrest in Pregnancy Algorithm guides clinicians step by step. It helps identify reversible causes, decide when to perform a perimortem cesarean, and apply pregnancy-specific modifications to resuscitation. When maternal arrest occurs at or beyond 20 weeks of gestation, performing a cesarean within four to five minutes can improve maternal circulation and give the fetus a chance to survive. Rapidly identifying the cause, following the algorithm, performing timely resuscitation, and providing post-arrest critical care all improve outcomes. Preparedness and teamwork are key to managing cardiac arrest during pregnancy.
Note: This cardiac arrest in pregnancy algorithm guideline is valid for 2025–2030
Cardiac arrest during pregnancy is rare but can be life-threatening. Acting quickly and following clear steps can save both mother and baby.
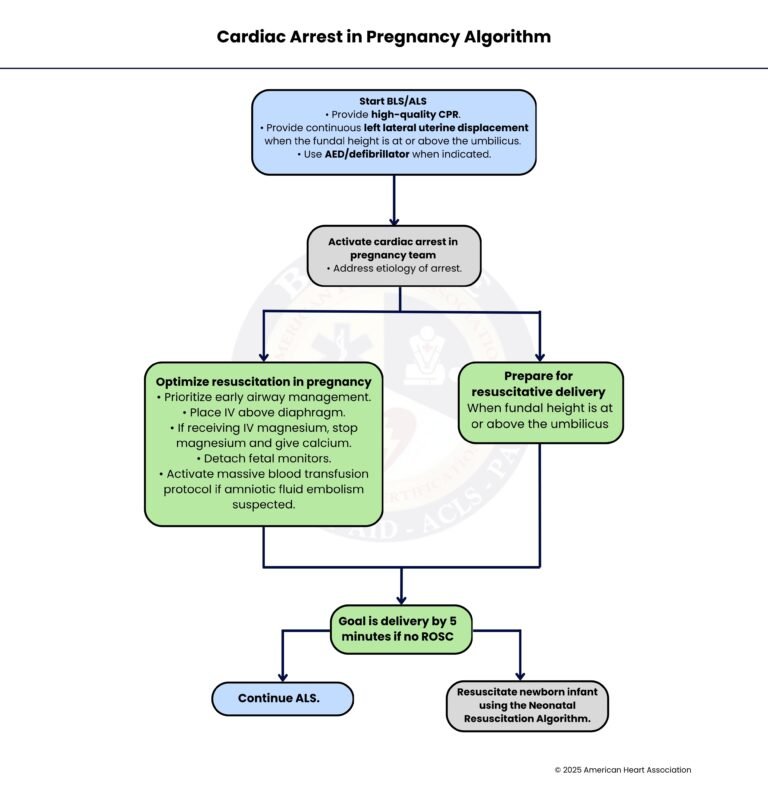
Immediately begin high-quality CPR, ensuring compressions are firm, fast, and uninterrupted. If the uterus has grown to or above the umbilicus, provide continuous left lateral uterine displacement to relieve pressure on the aorta and improve blood flow to the heart and brain. Use an AED or defibrillator if indicated to correct shockable rhythms.
Call for a specialized team including obstetric, anesthesia, and neonatal personnel. At this stage, it is important to identify the cause of the arrest. If the patient is still pregnant and needs resuscitation, move to Step 3. If the patient is undergoing delivery, go directly to Step 6.
Focus on pregnancy-specific considerations: secure the airway early, place IV (Intravenous) access above the diaphragm, and stop magnesium infusion if the patient was receiving it, giving calcium as needed. Remove fetal monitoring equipment to avoid interference, and if amniotic fluid embolism is suspected, activate the massive transfusion protocol. These steps maximize maternal circulation and address reversible causes.
If the mother does not achieve return of spontaneous circulation (ROSC) within about 4-5 minutes of arrest and the pregnancy is viable, the goal is to perform a perimortem cesarean delivery to improve maternal and fetal outcomes. If delivery is achieved, proceed to Step 7 to care for the newborn.
Maintain high-quality CPR, defibrillation, and appropriate medications while monitoring for ROSC. Continue addressing reversible causes and maintaining maternal oxygenation and circulation.
When the fundal height is at or above the umbilicus and delivery is indicated, prepare for rapid perimortem cesarean delivery. This step ensures the procedure can occur within the critical 4-5 minute window if maternal resuscitation is unsuccessful. After delivery, proceed to Step 7.
Once the baby is delivered, immediately follow the Neonatal Resuscitation Algorithm to support the infant’s breathing, circulation, and overall stability, ensuring both mother and child receive optimal care after the emergency.
During a cardiac arrest in pregnancy, a specialized team should be activated immediately. The exact members of this team may vary depending on the hospital or available resources. Usually, it includes a team leader who coordinates the resuscitation, an anesthesiologist to manage the airway and medications, an obstetrician to manage pregnancy-related issues and possible emergency delivery, and a neonatologist to care for the newborn if delivery occurs. Nurses assist with monitoring, medications, and equipment, while pharmacists help prepare emergency drugs. Other healthcare professionals may also participate depending on the situation. Having a coordinated team improves response time and patient outcomes.
In late pregnancy, the enlarged uterus can press on major blood vessels such as the aorta and inferior vena cava, which reduces blood flow to the heart and brain. This is called aortocaval compression. Left lateral uterine displacement means gently pushing the uterus toward the mother’s left side during CPR. This helps relieve the pressure on these blood vessels, allowing better blood circulation and making chest compressions more effective during resuscitation.
Resuscitative delivery (also called perimortem cesarean delivery) is performed when a pregnant patient in cardiac arrest does not respond to initial resuscitation. The main purpose is to improve the mother’s chances of survival by relieving pressure from the uterus on the heart and major blood vessels. This can improve circulation and the effectiveness of CPR. If performed quickly, it may also help save the baby’s life, but the primary goal is always to improve the mother’s outcome.
When cardiac arrest occurs in a pregnant patient with a uterus at or above the umbilicus (usually after about 20 weeks of pregnancy), the goal is to deliver the baby within 5 minutes of the arrest if there is no return of spontaneous circulation (ROSC). Performing delivery quickly helps reduce aortocaval compression and can significantly improve the effectiveness of resuscitation efforts. However, the exact timing may depend on the hospital’s available resources and personnel.
Pregnancy often makes airway management more difficult. Hormonal changes and swelling of airway tissues can make it harder to place breathing tubes. In addition, pregnant patients have increased oxygen demand and can develop low oxygen levels quickly. Because of this, airway management, such as endotracheal intubation or placement of a supraglottic airway device, should ideally be performed by the most experienced healthcare professional available to ensure the airway is secured safely and quickly.
Cardiac arrest during pregnancy is a rare but serious event, and it can occur due to several factors. Here are the main causes and other causes too:
Complications related to anesthesia used during labor or surgery can sometimes lead to cardiac arrest. These may include severe allergic reactions, medication overdose, or breathing problems caused by anesthesia.
Severe bleeding, such as postpartum hemorrhage or placental abruption, can cause significant blood loss. When the body loses too much blood, it can lead to shock and cardiac arrest if not treated rapidly.
Pregnant patients may experience heart-related conditions such as heart attack, cardiomyopathy, or severe arrhythmias. These cardiovascular problems can impair the heart’s ability to pump blood effectively and may lead to cardiac arrest.
Certain medications or drug reactions can cause cardiac complications, especially if there is an overdose or allergic reaction. Some drugs used in obstetric care may also affect heart rhythm or blood pressure if complications occur.
An embolism occurs when a substance blocks a blood vessel. In pregnancy, this may be caused by amniotic fluid embolism, where amniotic fluid enters the mother’s bloodstream, or pulmonary embolism, where a blood clot travels to the lungs. Both can rapidly lead to cardiac arrest.
Severe infections that cause high fever and sepsis can affect multiple organs and may eventually lead to cardiac arrest if not treated promptly.
Like other cardiac arrests, pregnancy-related arrest can also occur due to the general reversible causes known as the H’s and T’s. These include problems such as hypoxia (lack of oxygen), hypovolemia (low blood volume), electrolyte imbalance, thrombosis, toxins, and tension pneumothorax. Identifying and treating these causes is critical during resuscitation.
Severe pregnancy-related high blood pressure, such as preeclampsia or eclampsia, can lead to serious complications, including seizures, stroke, or organ failure. In severe cases, these conditions may result in cardiac arrest.
In summary, cardiac arrest during pregnancy is a rare but very serious emergency that needs fast action and clear teamwork. The Cardiac Arrest in Pregnancy Algorithm helps healthcare providers stay organized and focused during a stressful situation. By starting CPR quickly, adjusting resuscitation for pregnancy, and calling the right specialists, the team can improve the chances of survival for both mother and baby. Quick thinking, early airway care, and left uterine displacement support better blood flow during resuscitation. When the mother does not regain circulation, timely delivery may greatly improve the situation. Good preparation, regular training, and strong communication allow medical teams to respond with confidence and provide the best possible care in these critical moments.
Ready to save lives? Learn hands-on ACLS at Bayside CPR and gain the skills to confidently care for pregnant women in emergencies.
Cardiac arrest during pregnancy often happens because of pregnancy-related problems, such as severe bleeding, preeclampsia, or amniotic fluid embolism. Doctors must adjust CPR techniques, such as moving the uterus to the left and placing hands slightly higher on the chest.
Left lateral uterine displacement moves the uterus away from major blood vessels. This helps blood flow better to the heart and brain and makes chest compressions more effective.
Doctors aim to perform a perimortem cesarean delivery if the mother does not regain circulation within about 4–5 minutes of cardiac arrest and the pregnancy is at least 20 weeks. This step improves the mother’s circulation and may also help the baby survive.
The response team usually includes an obstetrician, an anesthesiologist, a neonatologist, nurses, and a team leader. Each member works together to manage resuscitation, airway care, possible delivery, and newborn care.
Common causes include severe bleeding, heart problems, embolisms, infections, and complications from anesthesia or medications. Doctors also check for reversible causes, such as low oxygen, low blood volume, toxins, and blood clots.
