
American Heart Association Training Center
The Basic Life Support (BLS) algorithm is used in emergencies such as cardiac arrest, choking, drowning, or any other situation, because these emergencies can occur suddenly, anywhere, and at any time. Every second without prompt action decreases the likelihood of survival. This algorithm offers a structured approach, guiding you from the moment you recognize an emergency to the delivery of effective CPR and defibrillation. It serves as a priority-driven, decision-making framework that directs each step of care. More than just a sequence of actions, it functions as an organized system that ensures your interventions remain efficient and coordinated, whether you are responding alone or as part of a well-trained team.
The BLS course covers the complete algorithm based on the 2025 AHA guidelines and aligns with the latest evidence-based standards. It also provides tailored approaches for adult and pediatric victims, as well as clinical procedures for a variety of scenarios you may encounter as a rescuer. Altogether, there are seven algorithms.

The basic life support algorithm guides people on how to act during medical emergencies when someone stops breathing or has a cardiac arrest. It helps rescuers respond in the right order so they can save lives more effectively.
The BLS Algorithm should be administered whenever there is a life-threatening medical emergency, especially involving the heart or lungs. These skills should be applied immediately to maintain body function until advanced medical help arrives and to improve the chance of survival. The primary situations that require BLS are:
Cardiac Arrest
BLS should be started as soon as the heart stops and there is no response. Chest compressions and rescue breaths keep oxygen circulating to the brain and other vital organs until advanced medical help arrives, greatly improving the chances of survival.
Respiratory Arrest
If breathing stops or is abnormal, BLS is crucial. Rescue breaths and proper airway positioning help maintain oxygen flow and prevent brain damage while waiting for emergency responders.
Airway Obstruction
When the airway is blocked and breathing is not possible, BLS techniques such as abdominal thrusts or rescue breaths can restore airflow. Prompt recognition and action are essential to prevent serious harm.
Drowning or Near-Drowning
In drowning situations, BLS should begin immediately, even if there is no response. Rescue breaths and chest compressions reintroduce oxygen to the lungs and help circulate blood until trained medical personnel take over.
Severe Choking
If coughing, speaking, or breathing is not possible due to choking, BLS interventions like abdominal thrusts and airway management are necessary. Acting without delay can clear the blockage and restore normal breathing.
Unresponsiveness Without Normal Breathing
Whenever there is unresponsiveness and abnormal or absent breathing, BLS must be started immediately. Early intervention sustains vital organ function and increases the likelihood of survival until professional help arrives.
Basic life support changes based on who needs help and the situation at hand. Understanding these special considerations helps you respond with the right actions and improve the chances of survival.
Adult CPR involves using two hands on the lower sternum to achieve a depth of at least 2 inches. For children and infants, techniques are adjusted for smaller bodies, using one hand or the two-thumb method with a target depth of about 1.5 inches. Since pediatric arrests are usually caused by respiratory issues, rescue breaths are prioritized more than in adult cardiac arrests. These differences are significant enough that the AHA provides a separate pediatric algorithm to ensure care meets the unique needs of younger patients.
Standard BLS applies to pregnant patients with two main adaptations. First, place your hands slightly higher on the sternum to accommodate the heart’s elevated position. Second, if a second rescuer is present, they should perform manual left uterine displacement by pushing the uterus to the left. When alone, maintain this adjustment by tilting the patient’s hips slightly to the left while performing compressions to support circulation during resuscitation.
In trauma-related cardiac arrest, controlling severe bleeding is a top priority alongside high-quality CPR. Apply direct pressure to major wounds without interrupting compressions. If spinal injury is suspected, stabilize the head and neck during the initial assessment, but do not reduce compression force, even if rib fractures are present. Effective compressions remain the most critical factor for survival, regardless of trauma.
For drowning victims, where respiratory arrest precedes cardiac failure, begin with five rescue breaths before chest compressions to restore oxygen promptly. In suspected opioid overdose, administer naloxone as soon as it is available, ensuring it is given alongside ongoing BLS rather than replacing it. In all cases, high-quality CPR is the essential foundation and must never be delayed or interrupted.
The 2025 AHA BLS guidelines introduce several important updates that aim to improve safety and effectiveness during emergencies. These changes simplify training, strengthen core skills, and help rescuers respond with more confidence in real situations.
Old (2020):
i. Adults & children: start with abdominal thrusts (Heimlich)
ii. Infants: alternate back blows and chest thrusts
New (2025):
i. Adults & children: 5 back blows → 5 abdominal thrusts, repeat until the object comes out
ii. Infants: 5 back blows → 5 chest thrusts, repeat (same as before)
Why it matters:
i. Back blows are safer and work better than abdominal thrusts alone.
ii. Makes training simpler because it’s now similar for all ages.
iii. Pregnant patients or when you can’t encircle the abdomen? Use 5 chest thrusts instead.
Impact: Fewer injuries from choking interventions in emergency settings.
2. Infant CPR – Hand Position Changes
Old (2020):
i. Primary: 2-finger technique
ii. Alternative: 2-thumb encircling hands or heel of 1 hand
New (2025):
i. Recommended: heel of 1 hand or 2-thumb encircling hands
ii. The 2-finger technique is no longer recommended
Why it matters:
i. Studies show 2-finger compressions are too shallow.
ii. Heel-of-1-hand or 2-thumb gives stronger, more consistent compressions.
Training note:
i. Use 2-thumb if multiple rescuers are present.
ii. Use heel-of-1-hand if you can’t encircle the infant’s chest.
3. Defibrillation Pads for Women
New (2025):
i. You can adjust a bra instead of removing it to place pads.
Why it matters:
i. Women are less likely to get public defibrillation.
ii. Adjusting instead of removing a bra reduces hesitation.
iii. Pads must still touch bare skin, but full removal isn’t always needed.
4. Mechanical CPR Devices
Old: unclear use
New (2025):
i. Do NOT use routinely for adult cardiac arrest.
ii. Can be used in special cases (prolonged transport, cath lab, ECPR prep) if manual compressions are difficult.
Why it matters:
i. Manual compressions work just as well, sometimes better.
ii. Devices only help when manual CPR is unsafe or impossible.
5. Ventilation During CPR
NEW Emphasis (2025):
i. Give enough air to see the chest rise.
ii. Avoid too little or too much ventilation.
iii. For respiratory arrest: 1 breath every 6 seconds (10/min).
iv. Standard 30:2 compression-to-ventilation ratio still applies before an advanced airway.
Why it matters:
i. Proper ventilation plus chest compressions improves survival.
6. CPR for Patients with Obesity
New (2025):
i. Use the same CPR techniques as everyone else.
Why it matters:
i. No evidence shows that modifications help.
ii. Ensures high-quality CPR for all adults.
7. Trauma and Airway Management
Updated (2025):
i. For adults with head/neck trauma:
ii. First try jaw thrust and airway device
iii. If the airway is still blocked → use head tilt-chin lift
Why it matters:
i. Opening the airway is the priority.
ii. Protecting the spine is important, but oxygenation comes first.
Information Source: Project Heartbeat
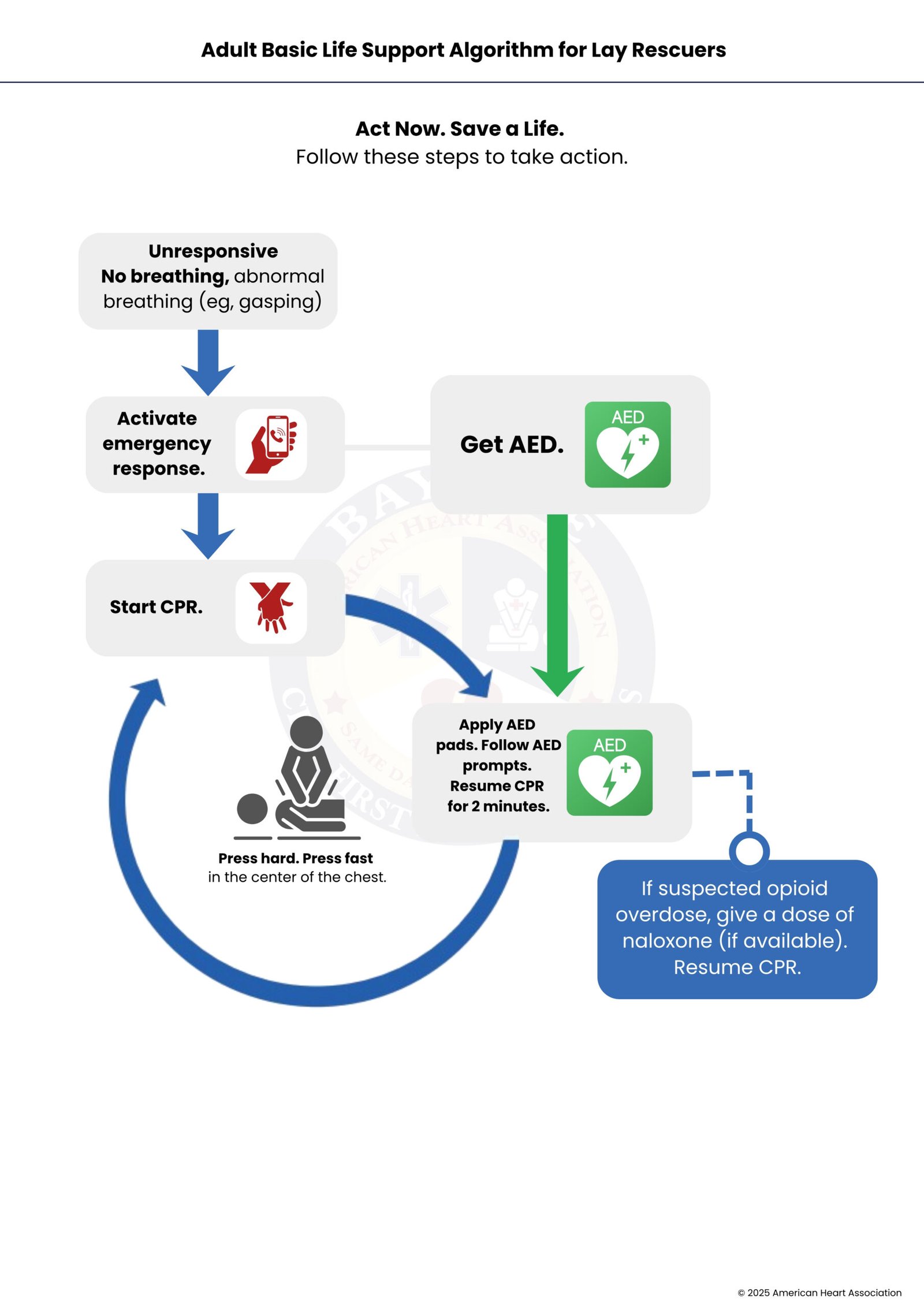
The Adult BLS Algorithm for Lay Rescuers is a structured approach to help a bystander provide immediate care to an adult who is unresponsive and not breathing normally (or not breathing at all) until professional help arrives. It’s designed to maximize survival from cardiac arrest by ensuring early recognition, early CPR, and early defibrillation.
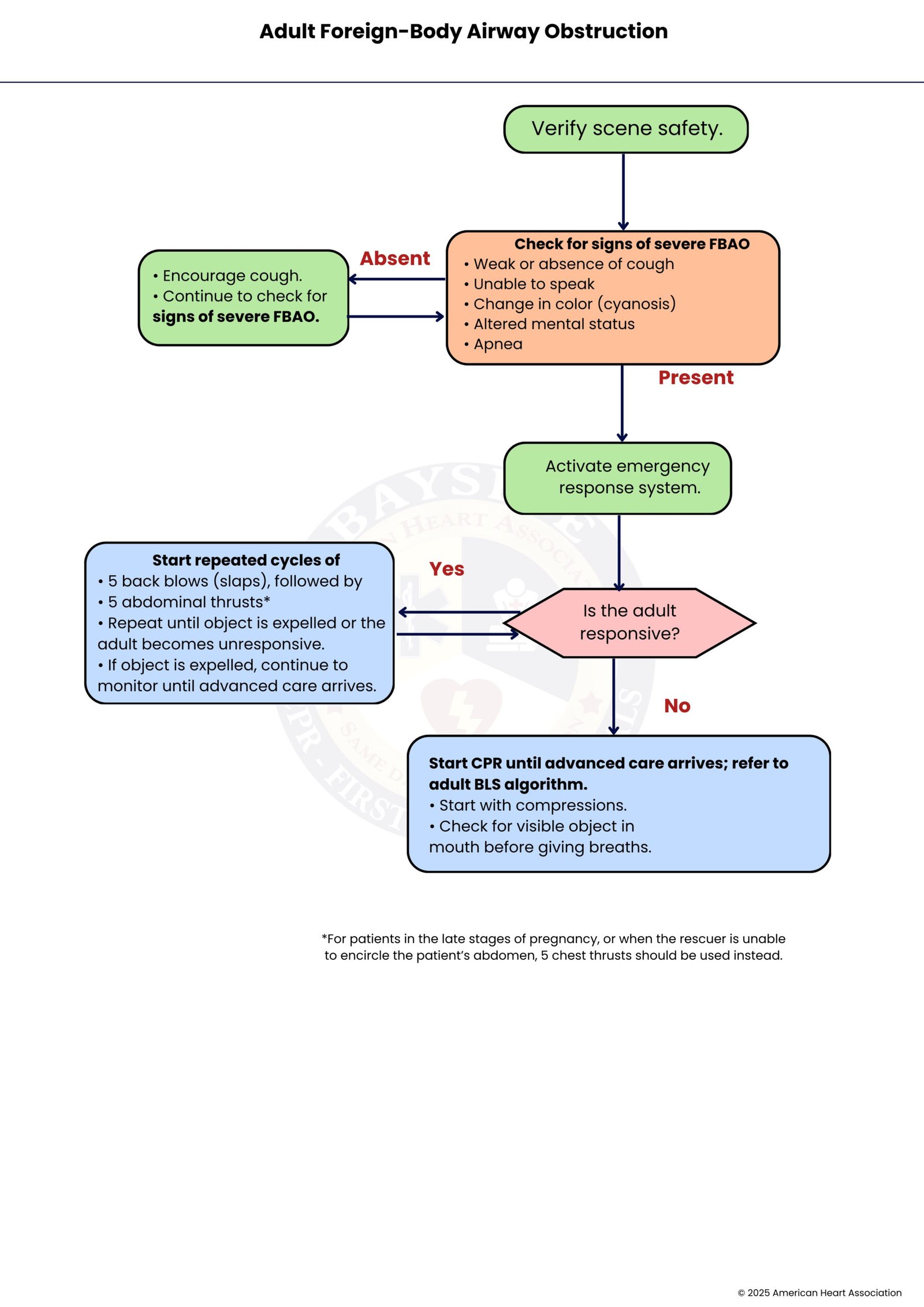
The Adult FBAO Algorithm is a step-by-step guide for responding to an adult who is choking due to a blocked airway, usually from food or another object. It helps a rescuer quickly relieve the obstruction and prevent life-threatening complications.
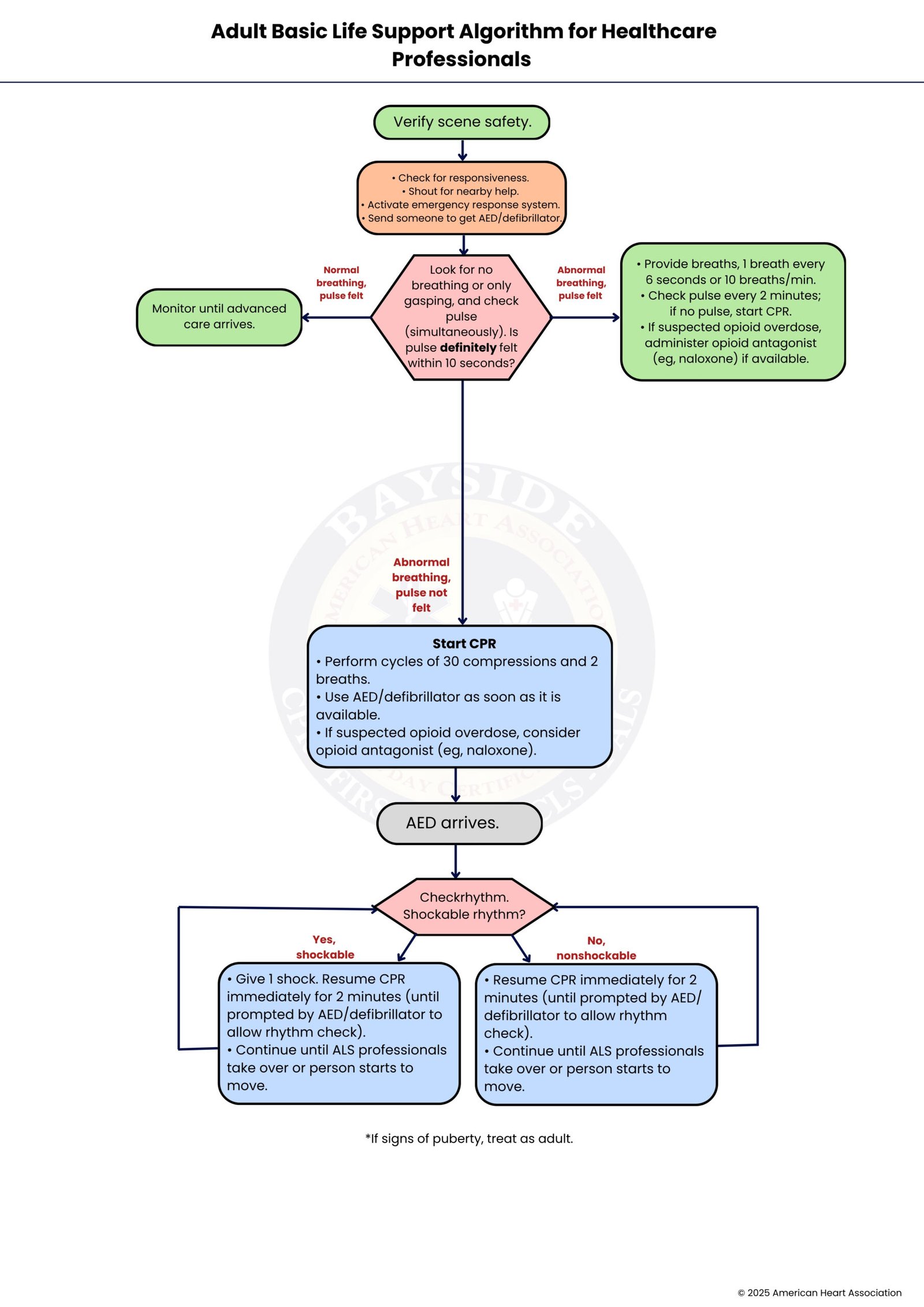
The Adult Basic Life Support (BLS) Algorithm for Health Care Professionals is a structured, evidence-based approach that guides trained medical personnel in the immediate management of an adult in cardiac arrest. It ensures rapid recognition, effective CPR, and early defibrillation, while allowing for advanced interventions when needed. This algorithm is more detailed than the lay rescuer version, as health care professionals are trained to monitor pulses, provide advanced airway management, and coordinate care with team members.
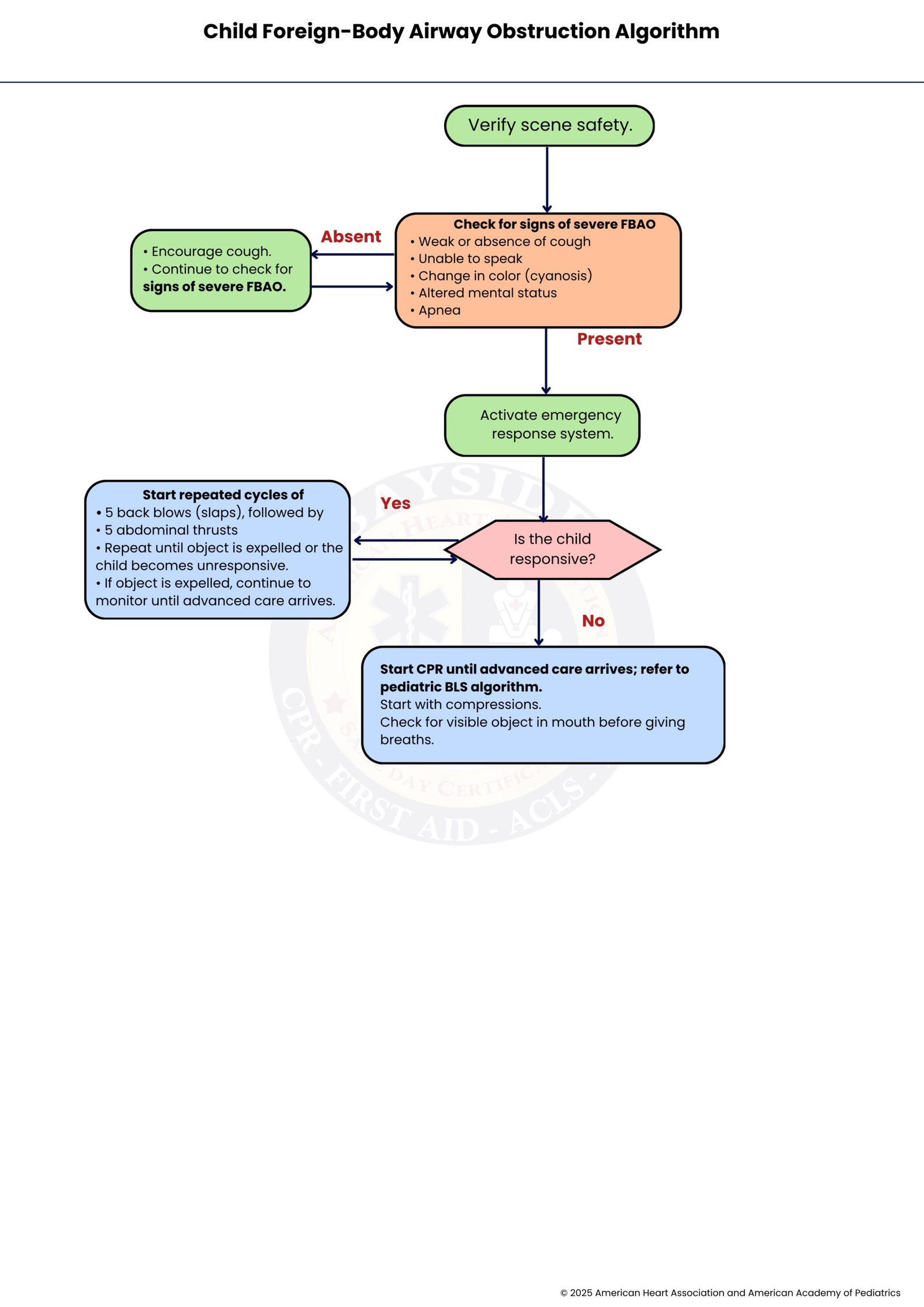
The Child FBAO Algorithm is a step-by-step guide for managing choking in children (ages 1 year to puberty) caused by food, small objects, or other foreign bodies. It helps rescuers quickly relieve airway obstruction and prevent life-threatening hypoxia or cardiac arrest.
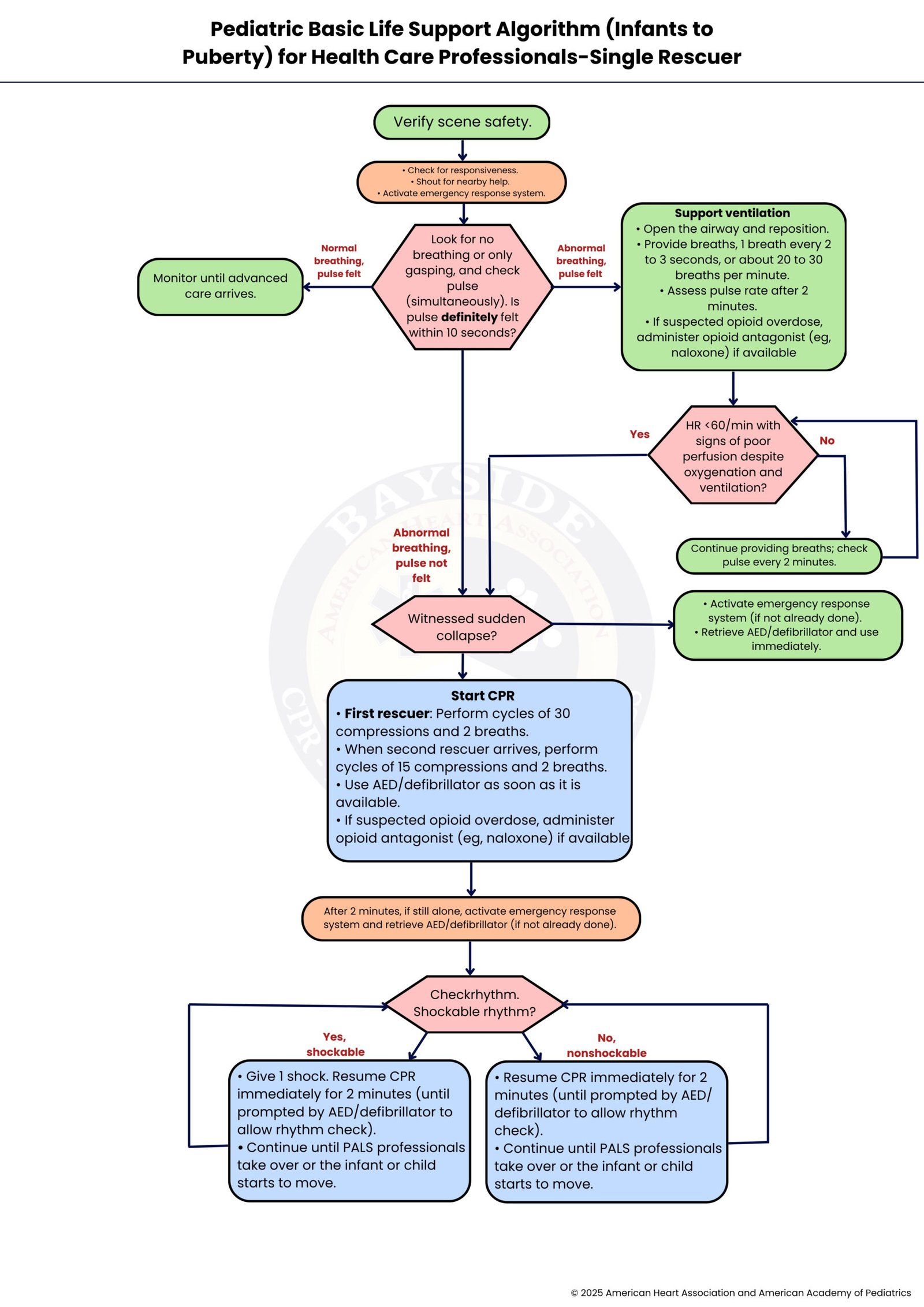
The Pediatric BLS Algorithm for Health Care Professionals—Single Rescuer is a structured approach to provide immediate care to a child or infant (from birth to puberty) who is unresponsive and not breathing normally. It guides healthcare providers to deliver timely, effective interventions that maintain circulation and oxygenation until advanced help arrives.
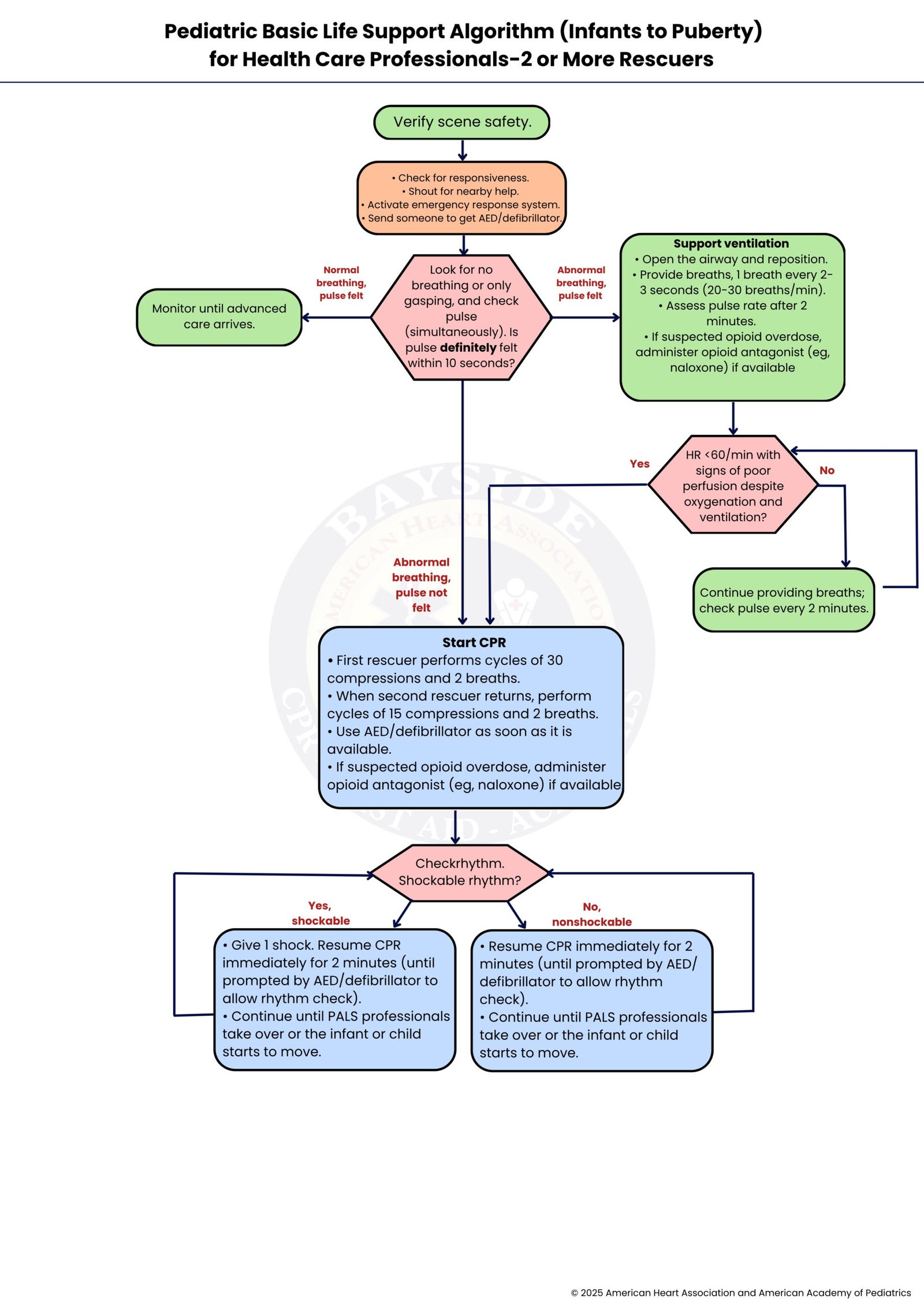
The Pediatric BLS Algorithm for Health Care Professionals—Two or More Rescuers is a structured approach for resuscitating infants and children (from birth to puberty) when multiple trained responders are available. It enables more effective, coordinated care, improving survival and outcomes by sharing tasks such as compressions, breaths, and emergency management.
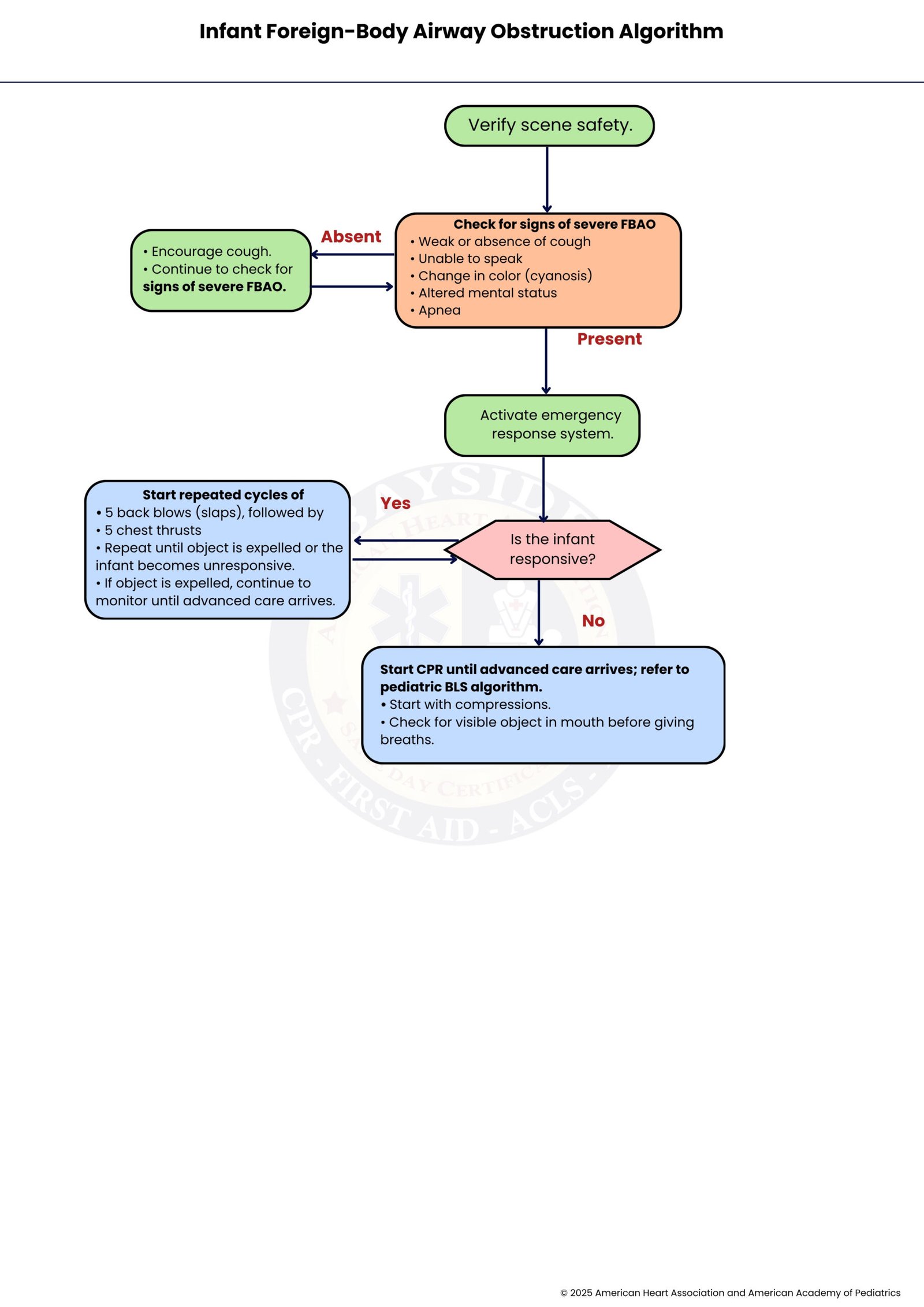
The Infant FBAO Algorithm is a step-by-step guide for rescuers to manage choking in infants under 1 year old, usually caused by food or small objects. It helps quickly relieve the airway obstruction and prevent life-threatening oxygen deprivation.
In short, the BLS algorithm is a practical guide that helps anyone act quickly and confidently in life-threatening emergencies. It breaks down complex steps into clear actions, ensuring that CPR, rescue breaths, and airway management are delivered effectively. By following the algorithm, both trained professionals and lay rescuers can maintain vital circulation and oxygenation, improving a person’s chance of survival until advanced help arrives.
The updates in the 2025 AHA guidelines make the techniques safer, simpler, and more effective for all ages and special situations. Knowing and practicing BLS gives you the tools and confidence to make a real difference. Enroll in our BLS course and gain the life-saving skills to respond confidently to adults and children alike.
Ensure the area is safe, then check if the person responds to you. If they don’t respond, call emergency services immediately and get an AED if one is nearby.
Push down on the chest 100–120 times per minute, about 5–6 cm deep, and give 2 rescue breaths after every 30 compressions. Keep going until the person recovers, professional help arrives, or you are too tired to continue.
Yes! With a child, you adjust your hand placement and compression depth based on their age. If there are two rescuers, switch to a 15:2 ratio (compressions to breaths) instead of 30:2. The good news is that the core steps—check, call, compress—remain the same.
Encourage them to cough first. If that doesn’t work, use abdominal or chest thrusts for adults and children. For babies under 1 year old, use back slaps and chest thrusts instead—never abdominal thrusts.
When two people respond together, one can perform chest compressions while the other provides rescue breaths and sets up the AED, helping maintain high-quality CPR. They can also switch roles to prevent fatigue, giving the patient a better chance of survival.
