
American Heart Association Training Center
Pediatric bradycardia with a pulse happens when a child’s heart beats slower than normal but still maintains a detectable pulse. In children, bradycardia usually signals an underlying problem, often caused by low oxygen, respiratory issues, or shock, rather than a primary heart condition. Because normal heart rates differ by age, what counts as bradycardia depends on the child’s stage of development; for example, a heart rate below 100 in an infant or below 60 in an adolescent is concerning.
When a child shows bradycardia, clinicians focus on checking for poor perfusion, such as pale or bluish skin, weak pulses, low blood pressure, delayed capillary refill, or changes in consciousness. The first step is to support the child’s airway and breathing, provide oxygen, and assist ventilation if needed. Clinicians then identify and treat the underlying cause, whether it’s hypoxia (low oxygen), hypothermia (low body temperature), or another issue.
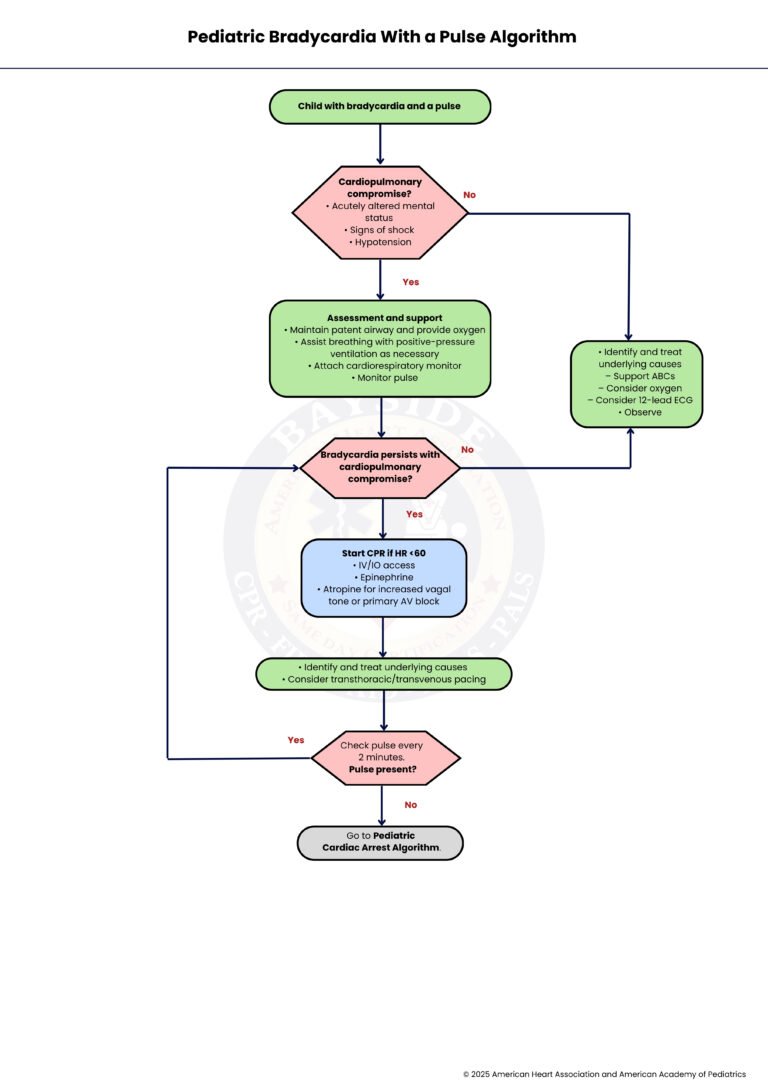
The Pediatric Bradycardia with a Pulse Algorithm guides this process, helping healthcare providers respond quickly and systematically. It shows when to focus on airway and breathing, when to use medications like epinephrine or atropine, and when to escalate care to advanced interventions. By following the algorithm, clinicians can act promptly to stabilize the child and prevent bradycardia from progressing to cardiac arrest.
Note: This pediatric bradycardia with a pulse algorithm guideline is valid for 2025–2030

Sometimes a child’s heart beats slower than normal, even though it still has a pulse. Understanding the main types helps spot the cause and guide care quickly.
Results from intrinsic cardiac issues affecting the heart’s pacemaker or conduction system, such as congenital heart block, myocarditis, or surgical injury to the conduction tissue.
Occurs due to systemic or non-cardiac causes that indirectly affect the heart rate, most frequently hypoxia, acidosis, hypotension, hypothermia, or medication effects.
In children who still have a pulse, it’s important to know what counts as a normal heart rate and when it is too low. These numbers help spot bradycardia quickly and guide care.
| Age Group | Normal Heart Rate (beats per minute) | Bradycardia Threshold (beats per minute) |
| Newborn (0–1 month) | 100–180 | <100 |
| Infant (1–12 months) | 100–160 | <100 |
| Toddler (1–2 years) | 90–150 | <90 |
| Preschool (3–5 years) | 80–140 | <80 |
| School-age (6–12 years) | 70–120 | <70 |
| Adolescent (13–18 years) | 60–100 | <60 |
Key Points:
– Bradycardia is defined as a heart rate below the normal range for the child’s age.
– Younger children naturally have faster heart rates, so thresholds vary with age.
– Always consider the child’s clinical condition; low heart rate may be normal in a sleeping child, but can be dangerous if there are signs of poor perfusion or respiratory distress.
Bradycardia in children can be scary, but quick recognition helps guide the right care. This step-by-step guide walks you through what to do when a child has a slow heartbeat with a pulse.
First, identify that the child has a slow heart rate (bradycardia) but still has a detectable pulse. The initial recognition is critical because interventions differ depending on whether the child has a pulse or not. Careful assessment of heart rate, age-appropriate vital signs, and overall clinical status should be performed.
Determine if the child is showing signs of acute cardiopulmonary compromise, such as altered mental status, hypotension, or signs of shock. If these are present, the bradycardia is considered life-threatening, and immediate intervention is needed (Step 3). If the child is stable without these features, the situation is less urgent, and observation and underlying cause assessment can be prioritized (Step 9).
If the child is unstable, begin supportive care immediately. Ensure the airway is open, provide supplemental oxygen, and assist ventilation with positive-pressure support if needed. Attach a cardiac monitor to continuously track heart rate and rhythm, and monitor the pulse closely. This stabilization step is vital before moving to advanced interventions.
After initial support, reassess the child. If the bradycardia has resolved and the child is stable, aggressive interventions may not be necessary (move to Step 9). If bradycardia persists along with signs of compromise, escalate to advanced life support measures (Step 5).
If the heart rate remains under 60 beats per minute (bpm) despite supportive measures, initiate CPR, or Cardiopulmonary Resuscitation while maintaining IV (Intravenous) or IO (Intraosseous) access. Administer medications such as epinephrine and consider atropine if increased vagal tone or primary AV(Atrioventricular) block is suspected. The goal is to support perfusion until the heart rate improves.
Evaluate for reversible causes of bradycardia (e.g., hypoxia, electrolyte imbalance, hypothermia). Depending on the severity and response, pacing, either transthoracic (through the chest wall/ribs) or transvenous (via veins), may be considered if the bradycardia does not respond to medications. Treating the root cause is essential for long-term stabilization.
During CPR and interventions, reassess the pulse every 2 minutes. If a pulse is present, return to Step 4 to evaluate whether bradycardia still causes compromise. This frequent reassessment ensures timely adjustments to therapy.
If at any point there is no detectable pulse, transition to the Pediatric Cardiac Arrest Algorithm. This algorithm guides full resuscitation, including advanced life support interventions, defibrillation if indicated, and continuous monitoring.
For a child with bradycardia but no signs of cardiopulmonary compromise, focus on identifying and correcting underlying causes. Support airway, breathing, and circulation (ABC) as needed, provide supplemental oxygen, consider obtaining a 12-lead ECG (Electrocardiogram), and closely observe. Intervention is based on the child’s evolving condition rather than immediate aggressive resuscitation.
Epinephrine is given when a child has bradycardia with poor perfusion that does not improve with oxygenation and ventilation. It works by increasing heart rate and improving cardiac output. The dose is 0.01 mg/kg (using a 0.1 mg/mL concentration), and it can be repeated every 3–5 minutes if needed, with a maximum single dose of 1 mg.
Atropine is used when bradycardia is caused by increased vagal tone or certain types of heart block. It helps by blocking vagal effects on the heart, allowing the heart rate to rise. The dose is 0.02 mg/kg, and it may be repeated once if necessary. The minimum dose is 0.1 mg, and the maximum single dose is 0.5 mg.
When a child’s body temperature drops too low, the heart rate slows down as metabolism decreases. Treating hypothermia by gently rewarming the child often helps correct the bradycardia.
This is the most common cause of pediatric bradycardia. Low oxygen levels cause the heart rate to slow as the body struggles to meet oxygen demands. Immediate airway support and oxygenation are critical and often resolve the problem.
Certain drugs or toxic exposures (such as beta-blockers or calcium channel blockers) can depress heart rate. Identifying and treating the specific toxin or reversing its effects is essential for recovery.
High pressure inside the skull can affect the brainstem, which controls heart rate, leading to bradycardia. This is often part of a serious condition and requires urgent management to reduce the pressure.
The vagus nerve can slow the heart rate when overstimulated, such as during suctioning, vomiting, or pain. This type of bradycardia is often temporary and may respond well to atropine.
Heart block occurs when electrical signals in the heart are delayed or blocked, leading to a slow heart rate. Depending on severity, treatment may include medications like atropine or even pacing.
Sometimes bradycardia is normal, such as in well-conditioned athletes or during sleep. In these cases, the child is stable and shows no signs of poor perfusion, so no emergency treatment is required.
In summary, pediatric bradycardia with a pulse is not just about a slow heart rate; it is a sign that something deeper may be wrong and needs quick attention. The key is to stay calm, assess the child carefully, and act step by step by supporting breathing, improving oxygen levels, and treating the cause. The algorithm gives a clear path that helps clinicians make safe and timely decisions without confusion. When providers follow this approach, they can stabilize the child, improve circulation, and reduce the risk of serious outcomes. With practice and awareness, this process becomes more natural and helps ensure better care for every child in need.
Ready to improve your skills in Pediatric Emergencies? Enroll in an AHA PALS course with Bayside CPR and boost your confidence in emergencies!
You can check the pulse by feeling the carotid artery in the neck or the brachial artery in infants. Do this gently and take no more than 10 seconds to decide.
Call for help right away if the child looks very weak, confused, or has trouble breathing. Fast action can prevent the condition from getting worse.
Yes, severe dehydration can slow the heart rate by affecting blood flow and oxygen delivery. Treating dehydration early can help improve the heart rate.
No, bradycardia is not always dangerous, especially during sleep or in active, healthy teens. It becomes serious only when the child shows signs of poor perfusion or distress.
Monitoring helps track changes in heart rate, breathing, and overall condition in real time. It allows caregivers to adjust treatment quickly if the child’s condition changes.
