
American Heart Association Training Center
The Pediatric Advanced Life Support (PALS) algorithm is a proven method developed by the American Heart Association (AHA) to guide healthcare providers in caring for critically ill or injured infants and children. It helps teams respond quickly during emergencies, such as respiratory failure, shock, or cardiac arrest.
PALS uses the Pediatric Assessment Triangle, appearance, breathing, and circulation, to quickly evaluate a child. Then it guides providers through clear steps: managing the airway, supporting breathing and oxygenation, giving chest compressions if needed, and using medications or defibrillation for certain heart rhythms. The approach emphasizes excellent CPR, fixing reversible problems, and continually reassessing the child to improve survival chances.

When a child faces a serious health problem, every second counts. PALS helps providers
In short, PALS reduces mistakes, supports teamwork, and gives providers a clear guide to save lives.
PALS is used whenever an infant or child has a condition that puts breathing, circulation, or neurological function at risk. It focuses on the critical time period where prompt, organized treatment can significantly improve survival and brain outcomes. The main situations that require PALS are:
If a child has no pulse or is not breathing, high-quality CPR should be started immediately. The Pediatric Cardiac Arrest Algorithm is used to guide rhythm management, as well as appropriate medications and interventions.
When a child shows an abnormal heart rate with signs of poor blood flow, it is important to assess whether the rhythm is contributing to the instability and then follow the correct PALS treatment pathway based on the rhythm type.
If a child is working harder to breathe, has unusual airway sounds, or is not ventilating properly, the underlying cause must be identified quickly. Early intervention can prevent progression to respiratory arrest, which often precedes cardiac arrest in children.
If the circulatory system cannot supply enough oxygen to the body’s tissues, immediate action is required. PALS helps identify different types of shock—such as distributive, hypovolemic, obstructive, and cardiogenic—and provides tailored fluid and medication treatments for each.
When shock is caused by infection, rapid treatment is essential to prevent worsening organ damage. PALS outlines a structured approach that includes early fluid resuscitation, appropriate use of vasopressors, and timely administration of antibiotics.
After return of spontaneous circulation (ROSC), care shifts from resuscitation to stabilization. PALS guides ongoing management of oxygenation, circulation, blood sugar levels, and temperature to support brain function and promote recovery.
The systematic approach to PALS offers a structured method for evaluating and treating critically ill pediatric patients. It emphasizes the rapid recognition of life-threatening conditions through a consistent, step-by-step process, helping ensure that essential actions are not overlooked in high-pressure situations.
In pediatric cardiac arrest (as in adult ACLS), clinicians often remember the “H’s and T’s” as a way to quickly identify and treat reversible causes of arrest. These are critical because addressing them can lead to return of spontaneous circulation (ROSC).
Hypoxia: Low oxygen; ensure airway, give oxygen, ventilate
Hypovolemia: Low blood volume; give IV/IO fluids
Hydrogen ion (acidosis): Acid-base imbalance; improve ventilation/perfusion
Hypo-/Hyperkalemia: Potassium imbalance; correct electrolytes
Hypothermia: Low body temperature; rewarm the pediatric patient
Tension pneumothorax: Air pressure in the chest compresses the lungs/heart; needle decompression
Tamponade (cardiac): Fluid around the heart; pericardiocentesis
Toxins: Drug/poison overdose; give antidotes and supportive care
Thrombosis: Clot (pulmonary/coronary); anticoagulation/thrombolysis
Trauma: Severe injury; control bleeding and treat injuries
Effectively using the PALS Algorithm involves more than simply memorizing its steps. It requires an understanding of key clinical principles that influence the quality of care provided during pediatric emergencies. These principles are relevant in all PALS situations, regardless of the specific algorithm being followed.
01.
Prompt identification of respiratory distress, shock, or cardiac arrest in pediatric patients greatly improves the chances of preventing progression to a more severe condition. Pay close attention to early, often subtle signs such as altered breathing patterns, changes in skin color, fluctuations in consciousness, and variations in muscle tone. Intervening during compensated shock or the early stages of respiratory distress provides the best opportunity to stabilize the child before decompensation occurs.
02.
Clear and effective communication among team members is essential to minimize errors during pediatric resuscitation. Closed-loop communication involves assigning tasks explicitly, confirming instructions aloud, and acknowledging completion. Establishing roles prior to starting resuscitation helps avoid duplication of efforts and ensures all critical tasks are completed, allowing the team to remain organized and focused in high-pressure situations.
03.
All PALS interventions should be tailored to the child’s age and weight. Drug dosages, defibrillation energy, and equipment sizes differ significantly between neonates and adolescents. When a patient’s weight is unknown, tools such as a length-based system like the Broselow tape should be used. Applying adult-based measurements to pediatric patients can lead to harm and reduce treatment effectiveness.
04.
It is important to ensure that appropriately sized pediatric equipment is available and prepared before initiating resuscitation. This includes correctly sized bag-mask devices, airway adjuncts, defibrillator pads, and endotracheal tubes. Improper equipment sizing can hinder airway management, compromise the quality of CPR, and increase the risk of complications during urgent care.
The latest guidance from the AHA focuses on improving how quickly and effectively clinicians respond during pediatric emergencies. These updates highlight practical steps that help teams act faster, monitor patients more closely, and support better recovery after cardiac arrest.
1. Epinephrine Timing – Give Early
i. What’s new: Give epinephrine as soon as possible in children with non-shockable cardiac arrest rhythms.
ii. Why it matters: Faster administration is linked to better survival and neurological outcomes.
iii. Practical takeaway: Don’t delay epinephrine while trying to get perfect IV access—focus on giving the drug quickly (within minutes if possible).
2. Hemodynamic Monitoring During CPR
i. What’s new: If an arterial line is available during CPR, aim for:
→ Infants: Diastolic BP ≥ 25 mmHg
→ Children ≥1 year: Diastolic BP ≥ 30 mmHg
ii. Why it matters: Higher diastolic pressures during CPR are linked to better survival with good brain function.
iii. Practical takeaway: Use real-time blood pressure readings to guide and improve CPR quality when monitoring is available.
3. ETCO₂ Monitoring – Use Carefully
i. What’s new: End-tidal CO₂ (ETCO₂) can help assess CPR quality, but:
→ Do NOT use a single cutoff (like 20 mmHg) to stop resuscitation.
i. Why it matters: Some patients survive even with lower ETCO₂ values.
ii. Practical takeaway:
→ Use ETCO₂ as one of several indicators
→ Never rely on it alone to decide when to stop CPR
4. Post-Arrest Blood Pressure Management
i. What’s new: After returning to circulation, maintain blood pressure above:
→ Systolic BP > 10th percentile for age
→ Mean arterial pressure > 10th percentile
ii. Why it matters: Low blood pressure after arrest is common and linked to worse outcomes.
→ Practical takeaway: Actively monitor and support blood pressure early after resuscitation to improve survival and recovery.
5. Neuroprognostication – Use Multiple Tools
i. What’s new: No single test can reliably predict neurological outcome after cardiac arrest.
ii. Approach: Use a combination of methods, such as:
→ Clinical exam
→ EEG (up to 72 hours)
→ Biomarkers
→ Imaging studies
iii. Why it matters: Single findings can be misleading.
iv. Practical takeaway: Avoid making early decisions based on just one test; assess over time using multiple sources of information.
6. Post-Arrest Recovery and Survivorship
i. What’s new: Survivors should be evaluated for long-term needs within the first year.
ii. Areas to assess:
→ Physical recovery and rehab needs
→ Cognitive and learning abilities
→ Emotional and psychological health
→ Family and caregiver support
iii. Why it matters: Recovery continues long after hospital discharge.
iv. Practical takeaway: Care should not stop at survival—long-term follow-up and support are essential.
Information Source: Project Heartbeat
These PALS algorithms help guide care for children during life-threatening emergencies in a clear and step-by-step way. They focus on quick action, careful checks, and the right treatment to support breathing, heart function, and recovery.
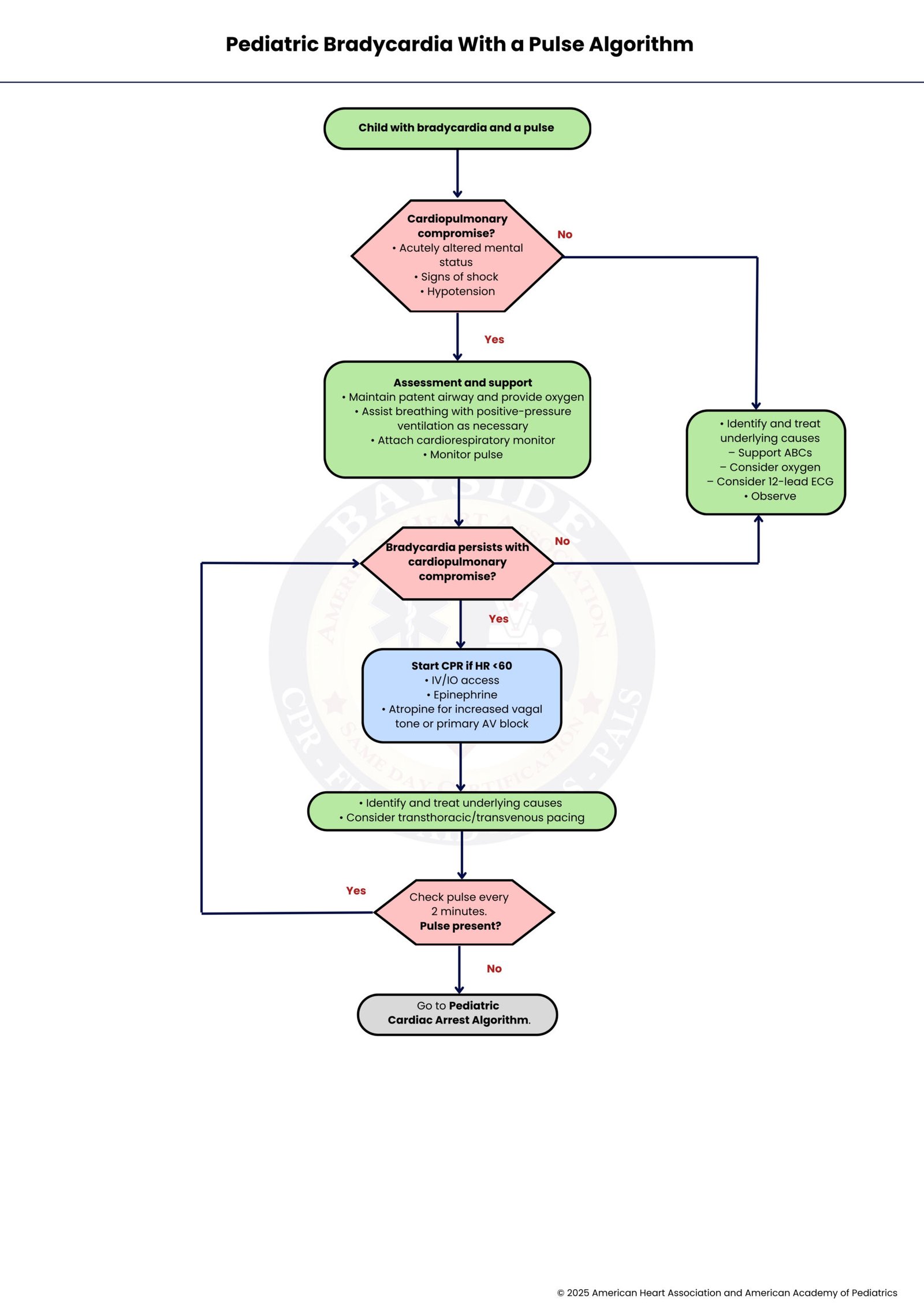
Pediatric bradycardia with a pulse is a heart rate below the age-specific normal range while a pulse is present, often due to hypoxia, shock, or systemic issues. The algorithm guides clinicians to assess perfusion, support the airway and breathing, provide oxygen, and assist ventilation. If the child remains unstable or HR < 60 bpm, CPR and medications like epinephrine or atropine are given. Frequent pulse checks, treating reversible causes, and escalating care as needed help stabilize the child and prevent progression to cardiac arrest.
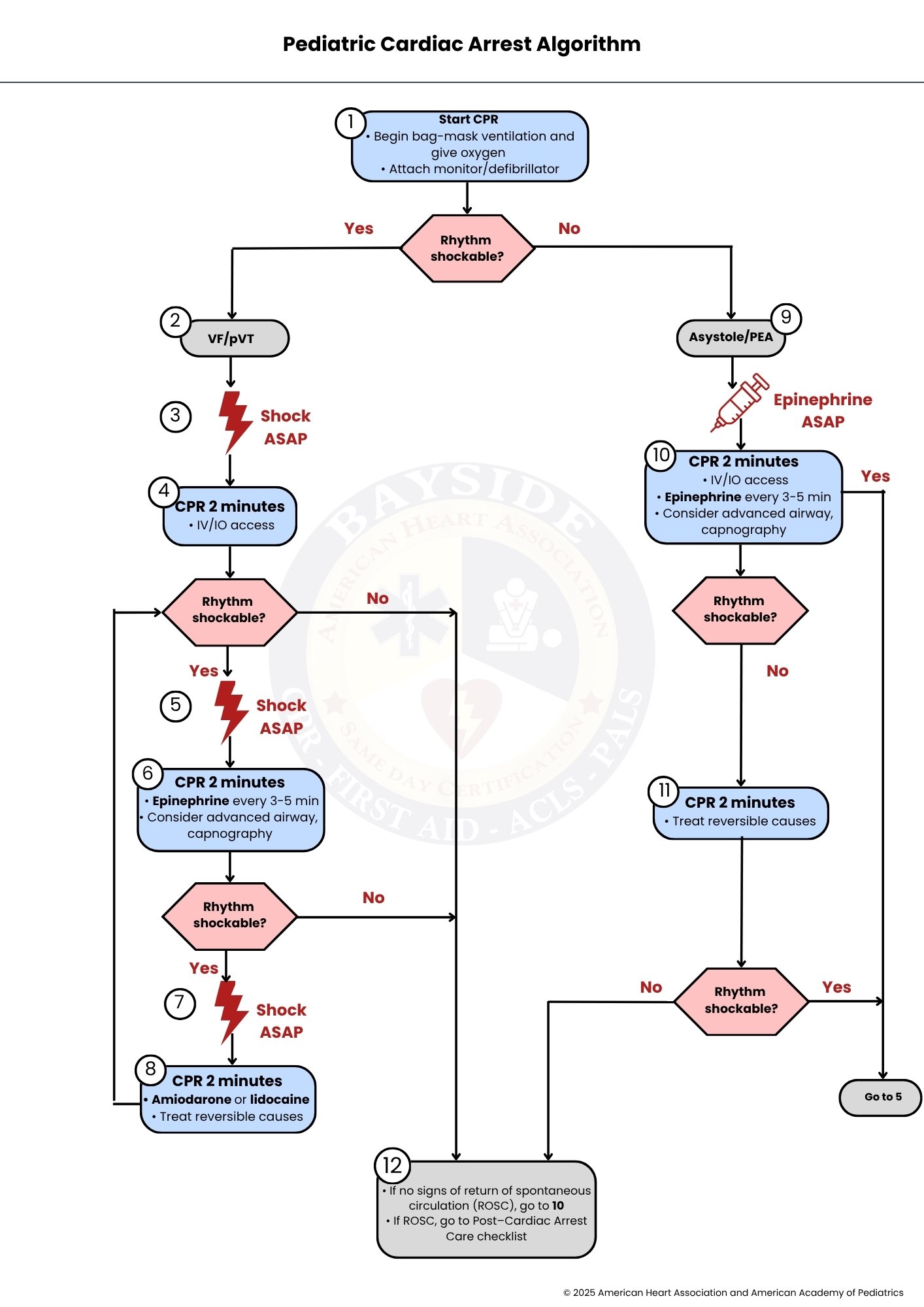
The Pediatric Cardiac Arrest Algorithm guides management of children in cardiac arrest. It includes recognizing arrest, starting high-quality CPR, assessing rhythm, and treating shockable rhythms with defibrillation and medications, while non-shockable rhythms focus on CPR, epinephrine, and reversible causes. Advanced airway care and post-resuscitation management help improve survival and neurological outcomes, forming the core of Pediatric Advanced Life Support (PALS).
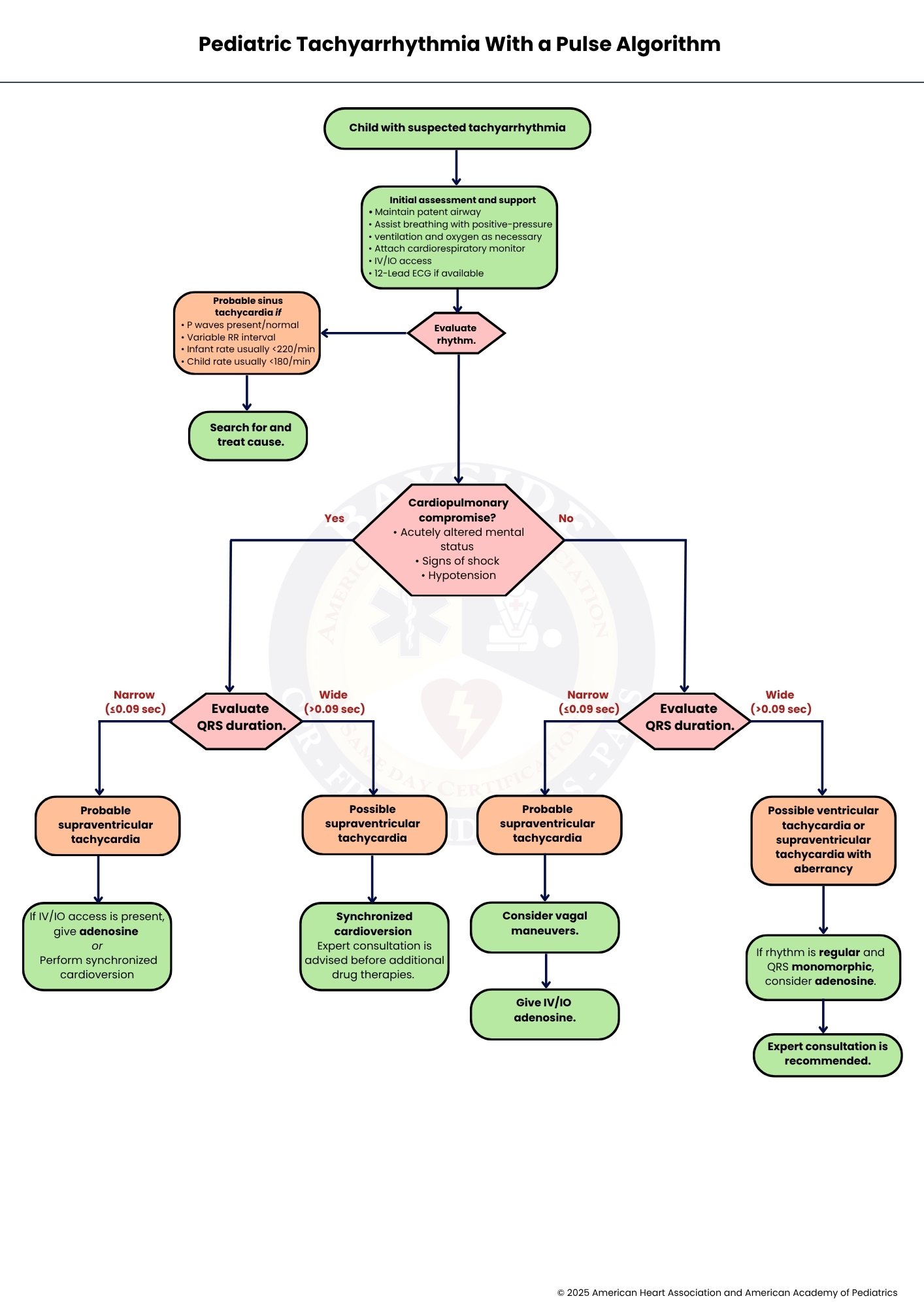
Pediatric tachyarrhythmia with a pulse is a rapid heart rate above age-specific norms with a detectable pulse. Management starts with assessing stability: unstable children need immediate cardioversion, while stable children may respond to vagal maneuvers or adenosine for SVT. ECG and QRS width help distinguish SVT from ventricular tachycardia, and underlying causes like infection, dehydration, or pain should be treated. Pediatric cardiology consultation is recommended for complex or refractory cases.

The Pediatric Post-Resuscitation Care Algorithm helps you know what to do after a child’s heart starts pounding again. It guides you step by step to keep them stable and safe. It’s like a care plan for their body and brain after CPR.

The Pediatric Septic Shock Algorithm shows you what to do when a child is in septic shock. It allows you to quickly assess, give fluids, and use medications to stabilize them. It’s a step-by-step plan to treat a serious infection and prevent it from getting worse.
“Note: AHA hasn’t updated the PALS Septic Shock Algorithm and Pediatric ROSC Post–Resuscitation Care Algorithm in 2025, so they still follow the 2020 guidelines.”
In short, the PALS algorithm gives healthcare providers a clear and simple way to care for children during serious emergencies. It helps them stay calm, act fast, and focus on what matters most to keep a child safe. By following these steps, teams can work better together, spot problems early, and give the right treatment at the right time. Regular practice also keeps skills fresh and builds confidence in high-pressure situations. Overall, PALS is not just a set of instructions; it is a reliable guide that supports better care and helps save young lives.
Sign up for the PALS course at Bayside CPR today. Begin the online portion whenever it suits you, then finish with a quick in-person skills session. Get fully AHA certified and be prepared to respond confidently in pediatric emergencies.
It usually takes practice over time, not just one course. Most people build confidence by reviewing cases, doing simulations, and using PALS regularly at work.
Yes, trained providers can use PALS in ambulances, clinics, or even during transport. The steps stay the same, but providers may need to adjust based on available equipment.
Stay calm and focus on the basics like airway, breathing, and circulation. Team members and cognitive aids, like cards or apps, can help guide you through the steps.
Yes, several mobile apps provide quick references, drug doses, and step-by-step guidance. These tools can support decision-making, especially in high-stress situations.
You should practice regularly, even between certification periods. Short, frequent practice sessions help you remember skills better and respond faster in emergencies.

