
American Heart Association Training Center
Adult post-cardiac arrest care is the treatment and support given to a person after their heart has started beating again following a cardiac arrest. Even when the heart begins to pump blood again, the brain and other organs may still be at risk because they did not receive enough oxygen during the arrest. This stage of care focuses on stabilizing the patient, protecting the brain, and treating the cause that led to the cardiac arrest. Health care teams closely monitor breathing, blood pressure, heart rhythm, and body temperature to help the body recover and prevent further damage.
The post-cardiac arrest care algorithm plays an important role in guiding medical teams through the steps needed after resuscitation. It provides a clear and organized plan that helps doctors and nurses make quick decisions during a critical time. By following the algorithm, the team can assess the patient, manage oxygen and blood circulation, control body temperature, and identify the underlying problem that caused the arrest. This structured approach improves coordination among the care team and increases the chances of survival and recovery for the patient.
Note: This adult post-cardiac arrest care algorithm guideline is valid for 2025–2030

Caring for someone after the heart starts beating again is a careful and organized process. This guide walks through the key steps that help doctors protect the brain, support the heart, and guide recovery.
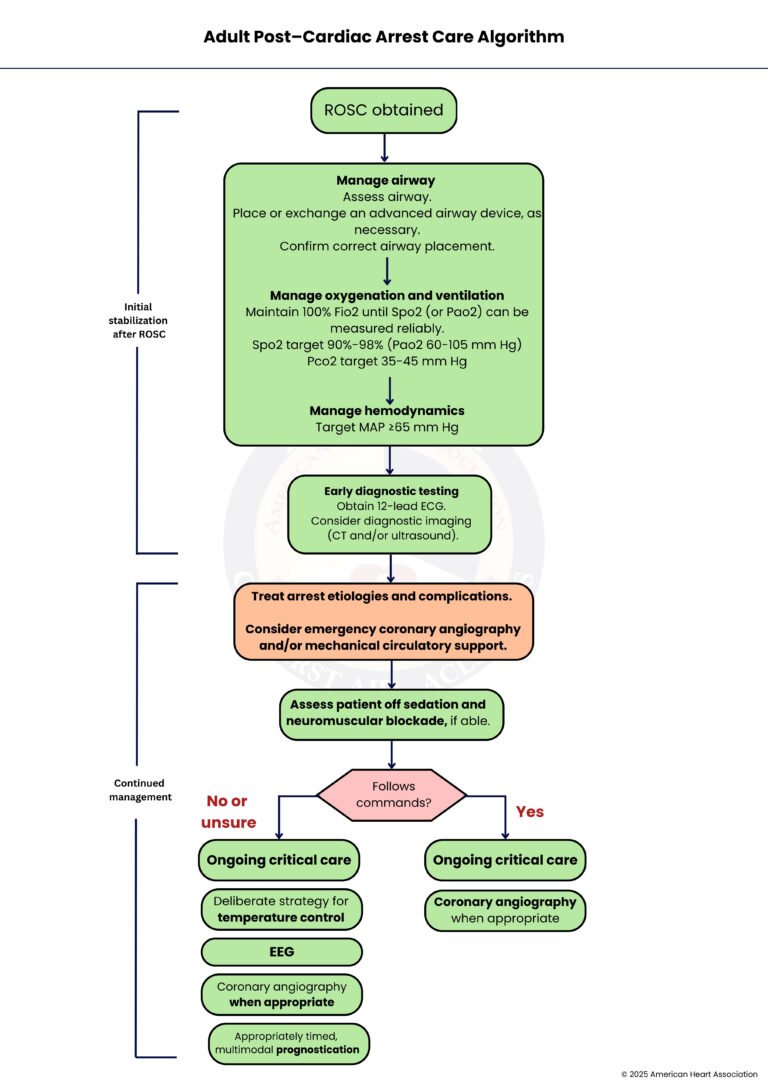
The first step is when the heart starts beating again after cardiac arrest. This moment is called the return of spontaneous circulation, or ROSC. It signals that emergency care has worked, and now the focus shifts to helping the body recover.
This is crucial to ensure that the brain and other vital organs receive the oxygen they need to function properly.
– Manage Airway
Check the airway carefully to make sure it is open. Place a new advanced airway device if needed, or replace the existing one. Confirm it is in the correct position to make sure the patient can breathe properly.
Maintain 100% FIO2 until SpO2 (or PaO2) can be measured reliably. Aim for SPO2 target 90% to 98% (PaO2 60 to 105 millimeters of mercury) and PCO2 target 35 to 45 millimeters of mercury. This helps the brain and other organs get enough oxygen while keeping carbon dioxide in a safe range.
– Manage Hemodynamics
Keep the mean arterial pressure (MAP) at or above 65 millimeters of mercury. This ensures that blood flows well to the heart, brain, and other vital organs to support recovery.
Get a 12-lead ECG (Electrocardiogram) to check the heart’s rhythm. Consider imaging tests such as a CT (Computed Tomography) scan or an ultrasound to find other problems that may have caused the arrest.
Identify and treat the underlying reason for the cardiac arrest. If needed, consider emergency procedures like coronary angiography to open blocked arteries or mechanical support to help the heart pump. It is a 30-to-60-minute minimally invasive procedure commonly used to diagnose chest pain, coronary artery disease, or heart valve issues.
If it is safe, stop sedation or muscle-blocking medications and see how the patient responds.
Check if the patient can follow simple commands. If yes, move to Step 12. If no or you are unsure, continue to Step 7.
Provide continuous care in the intensive care unit. Monitor vital signs closely, support organ function, and treat any new complications.
Use a deliberate strategy to control body temperature. This can protect the brain and improve recovery.
Perform an EEG, a safe, painless, non-invasive test that measures the brain’s electrical activity using electrodes placed on the scalp to detect seizures and assess brain function.
If a heart problem is suspected, perform coronary angiography to see and treat blocked arteries.
Use several methods to predict recovery. Look at neurological exams, imaging, and other tests to guide care decisions.
Continue intensive care support. Adjust treatments based on the patient’s progress and monitor closely.
Repeat coronary evaluation if needed to treat ongoing heart issues and support long-term recovery.
Surviving a cardiac arrest is only the first step in a patient’s recovery journey. What happens after the heart starts beating again, known as post-cardiac arrest care, plays a decisive role in determining whether a patient recovers fully, suffers long-term complications, or does not survive. Between 2025 and 2030, advancements in critical care continue to emphasize a structured, evidence-based approach to improve survival rates and neurological outcomes.
01.
Once circulation is restored, ensuring the body receives the right amount of oxygen becomes crucial. Both too little and too much oxygen can harm the brain. Modern care focuses on carefully adjusting oxygen levels to maintain safe saturation while also controlling carbon dioxide levels. This balanced approach helps prevent further brain injury and supports overall organ function during the critical recovery phase.
02.
After cardiac arrest, patients often experience unstable blood pressure, which can reduce blood flow to vital organs. Maintaining adequate blood pressure ensures that the brain and heart continue to receive sufficient oxygen and nutrients. Current guidelines stress the importance of closely monitoring and supporting circulation, often using fluids and medications to keep blood pressure within a safe range.
03.
One of the most important developments in post-cardiac arrest care is targeted temperature management. Patients who remain unconscious are often treated with controlled cooling or strict temperature regulation. This process reduces the brain’s metabolic demand and protects it from further damage. By preventing fever and maintaining optimal body temperature, healthcare providers can significantly improve neurological recovery.
04.
Understanding why the cardiac arrest occurred is essential to prevent it from happening again. Healthcare teams use diagnostic tools such as electrocardiograms, imaging, and blood tests to identify the root cause. Whether it is a blocked coronary artery, electrolyte imbalance, or another condition, timely and targeted treatment can be life-saving and reduce the risk of recurrence.
05.
Brain injury is one of the leading complications after cardiac arrest. Continuous neurological monitoring allows healthcare providers to detect seizures or other complications early. Advanced tools like EEG and regular clinical assessments help guide treatment decisions. Early intervention not only improves survival but also enhances the chances of meaningful neurological recovery, allowing patients to return to their daily lives.
– Resuscitation is ongoing during the post-ROSC phase, and many of these activities can occur concurrently.
– Manage Airway: Assess and consider placement or exchange of an advanced airway device (usually endotracheal tube or supraglottic device). Confirm the correct placement of an advanced airway. This generally includes the use of waveform capnography or capnometry.
– Manage Oxygenation and Ventilation: Titrate FIO2 for Spo2 90% to 98% (or PaO2 60 to 105 millimeters of mercury). Adjust minute ventilation to target PCO2 35 to 45 millimeters of mercury in the absence of severe acidemia.
– Manage Hemodynamics: Initiate or adjust vasopressors and/or fluid resuscitation as necessary for a goal mean arterial pressure of 65 millimeters of mercury or greater.
– Early Diagnostic Testing: Obtain a 12-lead ECG to assess for ischemia or arrhythmia. Consider CT head, chest, abdomen, and/or pelvis to determine the cause of arrest or assess for injuries sustained during resuscitation. Point-of-care ultrasound or echocardiography may be reasonable to identify clinically significant diagnoses requiring intervention.
1. Treat arrest etiologies and complications.
2. Consider emergency cardiac intervention:
– Persistent ST-segment elevation present
– Cardiogenic shock
– Recurrent or refractory ventricular arrhythmias
– Severe myocardial ischemia
3. Temperature control: If a patient is not following the commands of sedation and neuromuscular blockade or is unable to assess, initiate a deliberate strategy of temperature control with a goal of 32 °C to 37.5 °C as soon as possible.
4. Evaluate for seizure: Evaluate for clinical seizure and obtain an EEG to evaluate for seizure in patients not following commands.
5. Prognostication: Multimodal approach with delayed impressions (greater than or equal to 72 hours from ROSC or achieving normothermia).
6. Ongoing critical care includes the following:
– Target PaO2 60 to 105 millimeters of mercury, PCO2 35 to 45 millimeters of mercury (unless severe acidemia); avoid hypoglycemia (glucose less than 70 mg/dL) and hyperglycemia (glucose greater than mg/dL); target mean arterial pressure of 65 millimeters of mercury or greater.
– Consider antibiotics.
In short, adult post-cardiac arrest care plays a vital role in helping a patient recover after the heart begins to beat again. The care team follows a clear set of steps to protect the brain, support the heart, and keep the body stable during a very critical time. Careful monitoring of breathing, blood flow, and body temperature helps reduce further injury and gives the organs a better chance to heal. Doctors and nurses also work to find and treat the cause of the arrest so the problem does not happen again. When the team follows this organized approach, they can make faster decisions and provide better care. This process helps improve survival and gives patients a stronger chance for recovery and a better quality of life.
Want to sharpen your adult emergency skills? Join our hands-on ACLS course at Bayside CPR and become a confident, life-saving provider.
Yes, families can usually visit once the patient is stabilized in the ICU. Visits may be limited at first to reduce stress and infection risk.
Recovery time varies a lot depending on the patient’s health and how long the brain was without oxygen. Some people improve in days, while others need weeks or months of rehab.
Often, yes. Physical therapy helps the patient regain strength, coordination, and daily function after a serious event like cardiac arrest.
Some patients remember little or nothing about the event. Memory can be affected by brain oxygen levels, sedation, or medications used during treatment.
Yes, the risk is higher in the first days after ROSC. Doctors monitor the heart closely and may use medications, devices, or procedures to prevent another arrest.
