
American Heart Association Training Center
Adult bradycardia with a pulse occurs when an adult’s heart beats slower than 60 times per minute but still maintains a detectable pulse. Unlike cardiac arrest, the heart still pumps blood, though at a very slow rate, and may not deliver enough oxygen to the body. Heart disease, electrolyte imbalances, certain medications, or problems with the heart’s natural pacemaker (the sinoatrial node) can cause this condition. Patients may feel tired, dizzy, short of breath, or even faint, depending on how slow their heart beats. Recognizing the problem quickly and treating it properly can prevent serious complications such as low blood pressure, heart failure, or cardiac arrest. Well-conditioned athletes often have resting heart rates of 40-60 bpm, which can be normal.
The Adult Bradycardia with a Pulse Algorithm guides healthcare providers through assessing and managing patients with slow heart rates. It helps them check symptoms and vital signs, identify the cause, and decide on timely interventions. Providers may give medications like atropine, use pacing for severe cases, and continuously monitor the patient. Following this stepwise approach allows clinicians to act systematically and reduce the risk of complications.
Note: This adult bradycardia with a pulse algorithm guideline is valid for 2025–2030

Even in adults, a slower-than-normal heart rate can be concerning if the pulse is still present. Knowing the normal ranges helps identify bradycardia and guide timely care.
| Age Group | Normal Heart Rate (beats per minute) | Bradycardia Threshold (beats per minute) |
| Adults (18–60 years) | 60–100 | <60 |
| Older Adults (>60 years) | 60–100 | <60 |
Key Points:
– Bradycardia is defined as a heart rate below 60 beats per minute in most adults.
– Some healthy adults, especially athletes, may have a lower heart rate without problems.
– Always assess clinical signs, bradycardia with dizziness, low blood pressure, or poor perfusion requires urgent attention.
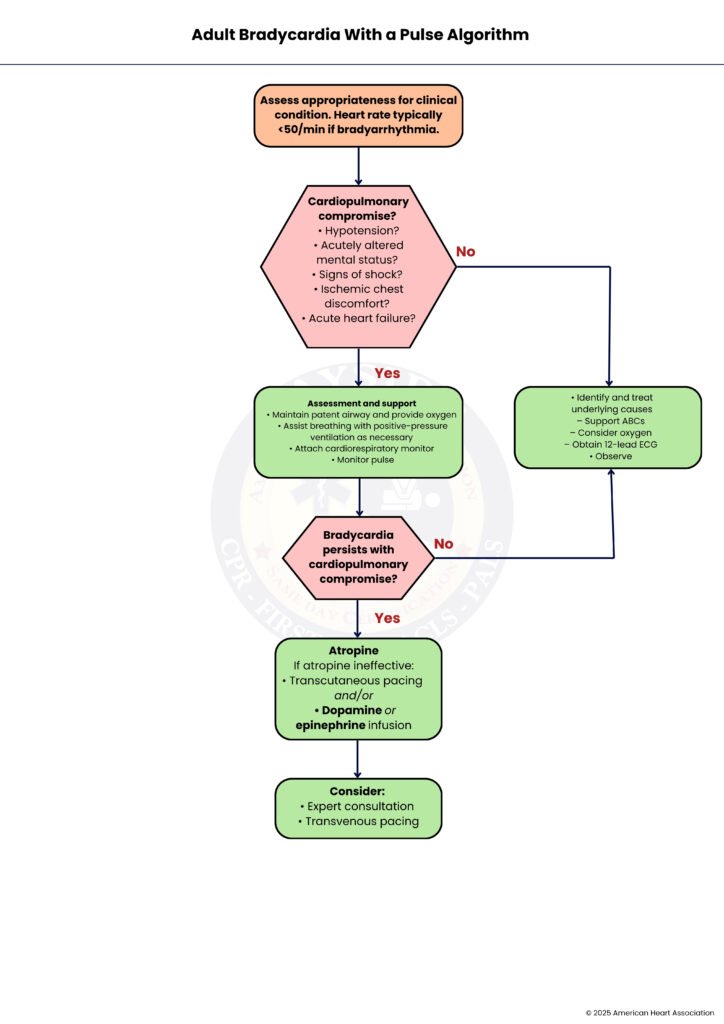
Bradycardia happens when the heart beats slower than normal and can cause serious problems. This guide walks you through the ACLS steps to recognize, support, and treat slow heart rates clearly and safely.
First, determine whether the patient truly has bradycardia. Clinically, bradycardia is usually defined as a heart rate below 50 beats per minute (bpm) in adults. Confirm that the slow heart rate is relevant to the patient’s current condition and not a normal variant, such as in athletes.
Evaluate whether the patient shows signs of poor perfusion or shock. Key indicators include low blood pressure (hypotension), acutely altered mental status, evidence of shock, ischemic chest discomfort, or acute heart failure. If any of these are present, immediate intervention is required (go to Step 3). If none are present, the patient may be stable, and observation or treatment of underlying causes can begin (Step 7).
Provide initial life support and monitoring. Ensure the airway is clear and give supplemental oxygen. Assist with breathing using positive-pressure ventilation if necessary. Attach a cardiac monitor to continuously assess heart rhythm and monitor the patient’s pulse to detect changes in bradycardia or signs of deterioration.
Determine if bradycardia continues despite initial support. If the slow heart rate persists and the patient remains compromised, escalate treatment to medications or pacing (Step 5). If the patient stabilizes, focus shifts to observation and underlying causes (Step 7).
Administer atropine as the first-line medication for symptomatic bradycardia. If atropine is ineffective, consider advanced interventions: transcutaneous pacing to maintain cardiac output, or continuous infusion of dopamine or epinephrine to support heart rate and blood pressure.
If bradycardia persists despite initial interventions, seek expert consultation. Consider transvenous pacing (TVP), which provides more stable and reliable heart rate support in critical situations and is usually performed by trained specialists.
For stable patients, focus on supportive care and diagnosis. Maintain airway, breathing, and circulation (ABCs), provide oxygen if needed, obtain a 12-lead ECG (Electrocardiogram), and investigate reversible causes such as medication effects, electrolyte imbalances, or ischemia. Continuous observation is essential to detect any deterioration.
Atropine is the first-line drug for symptomatic bradycardia. It works by blocking the vagus nerve’s effect on the heart, increasing heart rate. The recommended dose is 1 mg IV bolus, repeated every 3–5 minutes if needed. The maximum total dose is 3 mg. It is most effective for bradycardia caused by increased vagal tone or conduction block above the ventricles.
Dopamine is used when atropine fails or in cases of hypotension with bradycardia. It acts as a vasopressor and increases heart rate. The usual infusion rate is 5–20 micrograms/kg per minute, and it should be titrated based on the patient’s response. When discontinuing, taper slowly to prevent sudden drops in blood pressure or heart rate.
Epinephrine is a potent adrenergic agent used for persistent bradycardia with hemodynamic compromise. It is administered as an infusion at 2–10 micrograms per minute, adjusted according to the patient’s response. Epinephrine increases heart rate, cardiac contractility, and blood pressure, providing temporary support until definitive treatment is available.
Bradycardia can result from inadequate blood flow to the heart muscle, especially if the conduction system is affected. For example, inferior wall myocardial infarctions often involve the atrioventricular (AV) node, leading to slowed conduction and a low heart rate. Recognizing ischemia is critical because treating the underlying infarction may reverse the bradycardia.
Certain medications can slow the heart rate by affecting conduction or the autonomic nervous system. Common culprits include beta-blockers, calcium-channel blockers, and digoxin. Overdose or toxicity with these drugs can cause symptomatic bradycardia, requiring careful assessment, drug reversal if available, and supportive therapy.
Low oxygen levels in the blood can impair the heart’s ability to maintain a normal rate. Hypoxia can depress the sinoatrial node or AV conduction, resulting in bradycardia. Identifying and correcting hypoxia with supplemental oxygen or ventilatory support is essential for stabilization.
Abnormal levels of electrolytes, particularly hyperkalemia, can interfere with cardiac conduction and lead to bradycardia. Severe electrolyte disturbances may cause heart blocks or even cardiac arrest if untreated. Early recognition, laboratory testing, and correction of the imbalance are crucial.
In summary, adult bradycardia with a pulse requires careful assessment and timely action to keep the patient safe. A slow heart rate can sometimes be normal, but when it causes symptoms or poor blood flow, it becomes a serious concern. The Adult Bradycardia with a Pulse Algorithm helps healthcare providers respond in a clear and organized way. It guides them to check the patient’s condition, support breathing and circulation, give the right medicines, and use pacing when needed. It also reminds clinicians to search for the root cause so they can treat the problem and prevent it from returning. By following these steps, medical teams can make faster decisions, improve patient stability, and lower the risk of severe complications. Overall, the algorithm serves as a reliable guide that supports safe and effective care for adults experiencing bradycardia.
Build the confidence to act in adult bradycardia with a pulse emergency through Bayside CPR. Our flexible ACLS courses are for healthcare professionals who manage, direct, or respond to cardiopulmonary arrests and cardiovascular emergencies. This includes doctors, nurses, paramedics, and respiratory therapists working in emergency, critical care, or intensive care settings.
Adult bradycardia with a pulse happens when an adult’s heart beats very slowly, usually fewer than 60 beats per minute, but the heart still pumps blood. The body still gets some blood flow, but it may not be enough if the heart rate becomes too slow.
Bradycardia can make a person feel tired, dizzy, or short of breath. In more serious cases, it may cause chest pain or fainting.
The algorithm helps healthcare providers assess and treat patients with slow heart rates in a clear, step-by-step way. It guides them to check symptoms, give the right treatment, and monitor the patient closely.
Doctors usually give atropine first to treat symptomatic bradycardia. This medicine helps increase the heart rate by blocking signals that slow the heart down.
Many things can cause bradycardia, such as heart disease, low oxygen levels, medication effects, or electrolyte problems. Treating the underlying cause often helps improve the heart rate and the patient’s condition.
