
American Heart Association Training Center
Adult cardiac arrest is a life-threatening emergency that occurs when the heart suddenly stops pumping blood to the body. This sudden failure interrupts blood flow to the brain and other vital organs, causing immediate loss of consciousness and breathing. According to the American Heart Association (AHA), cardiac arrest is a major cause of death worldwide and can occur without warning, making it a critical medical emergency; every year, about 350,000 people die from cardiac arrest in the United States alone. Because survival depends heavily on how quickly treatment begins, a rapid and effective emergency response is essential. Immediate actions such as cardiopulmonary resuscitation (CPR) and defibrillation can significantly increase the chances of survival.
Advanced Cardiovascular Life Support (ACLS) provides healthcare professionals with evidence-based guidelines to manage life-threatening cardiovascular emergencies. These protocols are commonly used in hospitals, ambulances, and other emergency medical settings. This guide focuses on the ACLS Cardiac Arrest Algorithm, explaining the systematic steps healthcare providers follow to assess and treat cardiac arrest effectively.
Note: This ACLS cardiac arrest algorithm guideline is valid for 2025–2030

When someone’s heart suddenly stops, quick action can save their life. This guide walks you through the ACLS steps for cardiac arrest in a simple and clear way.
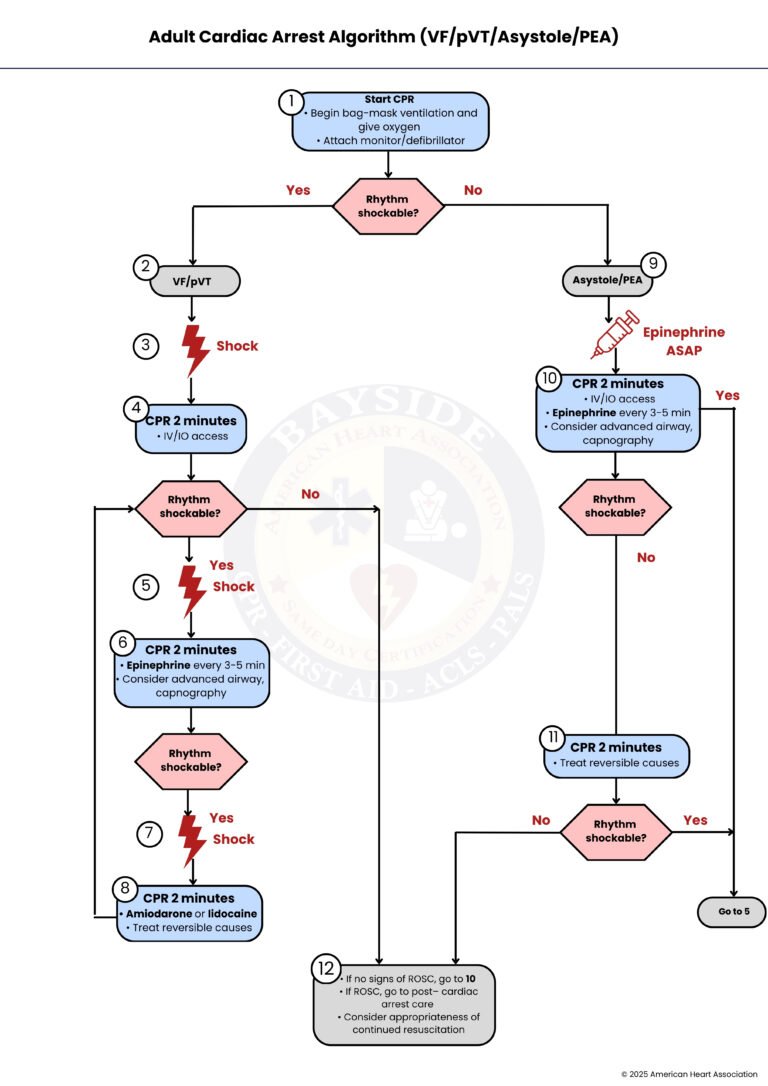
When an adult goes into cardiac arrest, start CPR immediately. Provide bag-mask ventilation with high-flow oxygen and attach a monitor or defibrillator to assess the heart rhythm. The first key decision is whether the rhythm is shockable. If it is, meaning ventricular fibrillation (VF) or pulseless ventricular tachycardia (pVT), follow the VF/pVT path starting at Step 2. If the rhythm is not shockable, meaning asystole or pulseless electrical activity (PEA), follow Step 9 instead.
If the rhythm is shockable (VF/pVT), you move to delivering a defibrillation shock. This is a critical step to try to restart the heart’s electrical activity.
Administer a shock as indicated by the defibrillator. The goal is to interrupt the abnormal rhythm and allow the heart’s natural pacemaker to take over.
After the shock, immediately resume CPR for 2 minutes. During this time, establish IV (Intravenous) or IO (Intraosseous) access. Reassess the rhythm: if it is still shockable, move to Step 5 to deliver another shock; if not, switch to the asystole/PEA pathway (Step 12).
Give a second shock if the rhythm remains VF/pVT. Quick defibrillation is essential to improve the chances of return of spontaneous circulation (ROSC).
Resume CPR for another 2 minutes. Administer epinephrine every 3 to 5 minutes and consider placing an advanced airway with capnography monitoring. After 2 minutes, check if the rhythm is shockable. If yes, go to Step 7; if no, proceed to Step 12.
If the rhythm is still shockable, deliver another shock. Continue rapid defibrillation cycles until the rhythm changes or ROSC is achieved.
After the shock, continue CPR for 2 more minutes and consider giving amiodarone or lidocaine to help stabilize the heart rhythm. Also, assess and treat any reversible causes like hypoxia, hypovolemia, or electrolyte imbalances.
If the rhythm is not shockable, such as asystole or PEA, give epinephrine as soon as possible. Immediate CPR remains the priority.
Continue CPR for 2 minutes while ensuring IV/IO access, giving epinephrine every 3 to 5 minutes, and considering an advanced airway with capnography. Reassess the rhythm: if shockable, go back to Step 5; if not, move to Step 11.
Resume CPR for another 2 minutes while addressing any reversible causes of the arrest (the “H’s and T’s”). Recheck the rhythm: if it becomes shockable, return to Step 5; if not, proceed to Step 12.
If there are no signs of ROSC, repeat the CPR and medication steps in Step 10. If ROSC occurs, transition to post–cardiac arrest care, including monitoring, hemodynamic support, and treating underlying causes. Always consider whether continued resuscitation is appropriate based on the patient’s condition.
Defibrillation is used to treat shockable cardiac arrest rhythms such as VF and pVT. The amount of energy delivered depends on the type of defibrillator being used.
For biphasic defibrillators, the recommended shock energy depends on the manufacturer’s guidelines. The initial shock is usually between 120 and 200 Joules. If the exact recommendation is unknown, the maximum available energy should be used. For the second and subsequent shocks, the same energy level or a higher energy dose may be used if necessary.
For monophasic defibrillators, the recommended defibrillation energy is 360 Joules per shock.
During adult cardiac arrest, medicines help the heart work better and improve blood flow. Giving the right medicine at the right time can save lives.
Epinephrine is given during cardiac arrest to improve blood flow to the heart and brain. The recommended IV or IO dose is 1 mg every 3-5 minutes throughout resuscitation.
Amiodarone is used for shock-resistant VF or pVT. The first dose is 300 mg IV/IO bolus. If a second dose is needed, give 150 mg IV/IO.
Lidocaine is an alternative antiarrhythmic for VF/pVT. The first dose is 1-1.5 mg/kg IV/IO. If a second dose is required, give 0.5-0.75 mg/kg IV/IO.
An advanced airway can be established using endotracheal intubation or a supraglottic airway (like a laryngeal mask airway). This allows for continuous chest compressions during CPR without pausing for breaths.
After placing an advanced airway, use continuous waveform capnography or capnometry to confirm correct tube placement and to monitor ventilation. Capnography also helps assess CPR quality and detect ROSC.
Identifying reversible causes is a vital step in managing cardiac arrest. These conditions may increase the likelihood of patient survival if identified in time. The Hs and Ts framework categorizes these reversible causes. These include:
Recognizing and treating these reversible causes can significantly improve resuscitation results. Detecting these factors early in the disease can guide treatment decisions and even save lives.
In summary, managing adult cardiac arrest requires quick action and careful attention. Following the ACLS algorithm helps healthcare providers respond step by step, whether the heart rhythm is shockable or not. Starting CPR without delay, giving defibrillation when needed, using medications correctly, and addressing reversible causes all work together to give patients the best chance of survival. High-quality compressions, proper airway management, and continuous monitoring make each step more effective. By acting fast and following these guidelines, rescuers can make a real difference and help the heart restart, giving patients the opportunity for recovery. Sign up for ACLS classes today and build the confidence to lead during emergencies. It’s more than just earning a course completion card; it’s a commitment to saving lives.
Start CPR immediately and make sure the person is breathing and unconscious. Attach a monitor or defibrillator to check the heart rhythm as fast as possible.
Shockable rhythms are ventricular fibrillation (VF) and pulseless ventricular tachycardia (pVT). You treat them by delivering a defibrillation shock and continuing CPR in cycles.
Give epinephrine as soon as possible and keep doing CPR without delay. Also, check for reversible causes like low oxygen, bleeding, or blocked arteries.
Medicines like epinephrine improve blood flow to the heart and brain, while amiodarone or lidocaine help stabilize the heart rhythm. Giving the right medicine at the right time can increase survival chances.
Good CPR pushes blood to the brain and heart, giving the patient the best chance to survive. This means pushing hard and fast, letting the chest fully recoil, and minimizing pauses during compressions.
