
American Heart Association Training Center
Pediatric cardiac arrest refers to the sudden cessation of effective heart function, breathing, and circulation in infants and children, leading to an immediate life-threatening emergency. Unlike adults, cardiac arrest in children is more commonly caused by respiratory failure, shock, or underlying medical conditions rather than primary heart disease. Rapid recognition and timely intervention are critical because survival depends heavily on early, high-quality resuscitation.
The Pediatric Cardiac Arrest Algorithm is a structured clinical guideline used by healthcare providers to standardize the management of cardiac arrest in children. It provides a step-by-step approach to ensure rapid assessment, effective cardiopulmonary resuscitation (CPR), appropriate airway and breathing management, medication administration, and identification of reversible causes. By following this algorithm, medical teams can reduce errors under pressure, improve coordination, and increase the chances of return of spontaneous circulation (ROSC) and survival with good neurological outcomes.
Note: This pediatric cardiac arrest algorithm guideline is valid for 2025–2030

Identifying pediatric cardiac arrest quickly can significantly impact results. Below are key signs to look for:
When handling pediatric cardiac arrest, several key considerations must be taken into account, including anatomical and physiological differences, team dynamics, and the importance of family support.
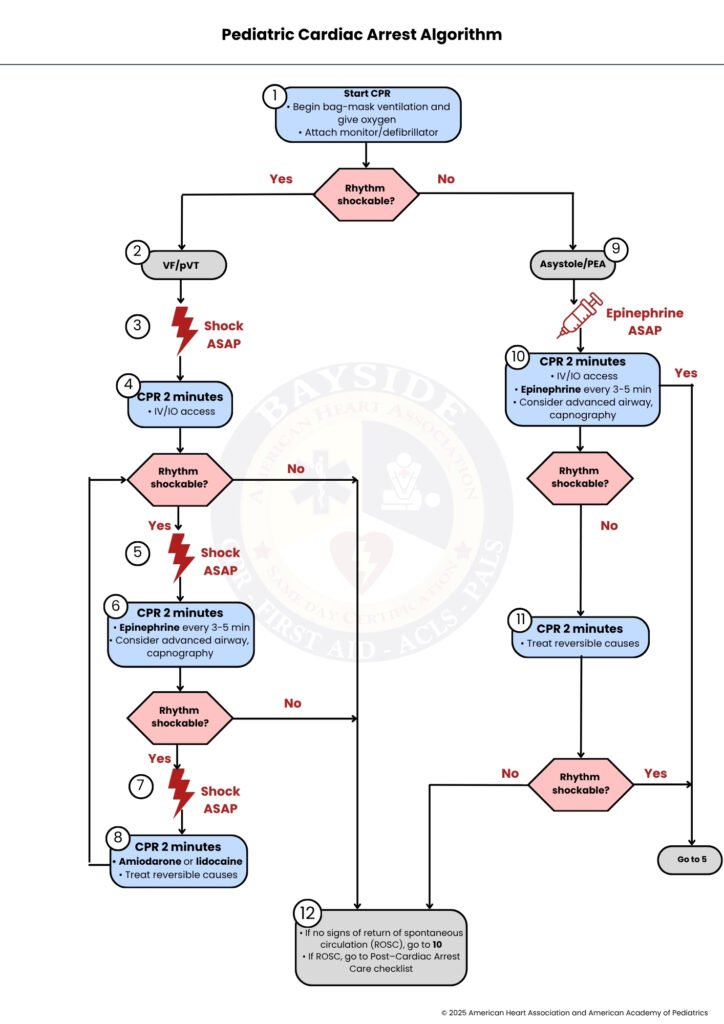
Let’s break down this algorithm step by step, so it will guide you through each part in a simple way.
Start CPR immediately once cardiac arrest is recognized. Begin high-quality chest compressions without delay and provide bag-mask ventilation with 100% oxygen to ensure adequate oxygen delivery. Attach a cardiac monitor/defibrillator as soon as possible to assess the heart rhythm. Once the rhythm is identified, determine whether it is shockable or nonshockable. If the rhythm is shockable, proceed to Step 2; if it is nonshockable, proceed to Step 9.
Perform CPR for 2 minutes while administering antiarrhythmic drugs such as amiodarone or lidocaine to stabilize the cardiac rhythm. Actively identify and treat reversible causes of cardiac arrest (such as hypoxia, hypovolemia, hydrogen ion imbalance, or electrolyte disturbances). Reassess rhythm after 2 minutes; if shockable, return to Step 5; if nonshockable, proceed to Step 12.
The patient is in a nonshockable rhythm, such as asystole or pulseless electrical activity (PEA). Administer epinephrine as soon as possible to improve perfusion and increase the chances of ROSC. Continue immediate CPR without interruption while focusing on identifying reversible causes. Proceed to Step 10.
Continue CPR for 2 minutes while maintaining high-quality compressions and establishing or maintaining IV/IO access. Administer epinephrine every 3 to 5 minutes and consider advanced airway placement with capnography for ventilation monitoring. After 2 minutes, reassess rhythm; if shockable, proceed to Step 5; if nonshockable, proceed to Step 11.
Continue CPR for another 2-minute cycle while actively treating reversible causes of arrest. Focus on correcting underlying issues such as hypoxia, hypovolemia, acidosis, or electrolyte imbalance. After reassessment, if the rhythm becomes shockable, proceed to Step 5; if it remains nonshockable, proceed to Step 12.
This step depends on the patient’s response. If there are no signs of return of spontaneous circulation (ROSC), continue resuscitation and return to Step 10 for ongoing advanced life support. If ROSC is achieved, immediately transition to post–cardiac arrest care, including stabilization, monitoring, and treatment of the underlying cause to prevent recurrence.
This sidebar provides critical drug dosages and CPR specifications as outlined in the 2025 guidelines.
i. Push hard: At least one-third of the anteroposterior diameter of the chest.
ii. Push fast: 100 to 120 compressions per minute.
iii. Allow complete chest recoil.
iv. Minimize interruptions: Aim for under 10 seconds.
v. Change the compressor every 2 minutes, or sooner if fatigued.
vi. Ventilation (No Advanced Airway):
– 15:2 ratio (2 or more rescuers, prepuberty)
– 30:2 ratio (2 or more rescuers, postpuberty onset)
– 30:2 ratio (single rescuer, any age)
vii. Ventilation (With Advanced Airway): Continuous compressions with a breath every 2 to 3 seconds (20-30 breaths/min).
viii. Monitor: ETCO₂ and, when available, invasive diastolic blood pressure.
i. First shock: 2 Joules per kilogram.
ii. Second shock: 4 Joules per kilogram.
iii. Subsequent shocks: At least 4 J/kg, up to a maximum of 10 J/kg or the adult dose.
i. Epinephrine IV/IO dose: 0.01 mg/kg (of 0.1 mg/mL concentration). Max single dose: 1 mg. Repeat every 3-5 minutes.
ii. Amiodarone IV/IO Dosis: 5 mg/kg bolus (max 300 mg). May repeat up to 2 times (max single dose 150 mg for subsequent doses).
iii. Lidocaine IV/IO dose: 1 mg/kg bolus.
i. Endotracheal intubation or supraglottic advanced airway.
ii. Waveform capnography or capnometry to confirm and monitor ET tube placement.
H’s: Hypovolemia, Hypoxia, Hydrogen ion (acidosis), Hypoglycemia Hypokalemia or hyperkalemia, Hypothermia
T’s: Tension pneumothorax, Tamponade, cardiac, Toxins, Thrombosis (pulmonary), Thrombosis (coronary)
In short, the pediatric cardiac arrest algorithm gives healthcare providers a clear and reliable path to follow during one of the most critical emergencies in children. It brings structure to a fast moving situation and helps teams act quickly, stay organized, and deliver the best possible care. By focusing on early recognition, strong CPR, timely medications, and treating the root cause, providers can greatly improve a child’s chance of recovery. Just as important, good teamwork and calm communication make a real difference when every second counts. When this approach is used with skill and care, it not only supports survival but also helps protect the child’s future health and quality of life.
Enroll in a PALS course today at Bayside CPR and be ready to make a life saving difference.
You should start CPR right away as soon as you recognize cardiac arrest. Begin chest compressions and give oxygen while you call for help and attach a monitor.
You check the heart rhythm using a monitor or defibrillator. If you see VF or pulseless VT, you give a shock immediately.
You restart CPR right away without stopping. Then you continue CPR for about 2 minutes before checking the rhythm again.
Epinephrine is given every 3 to 5 minutes to help improve blood flow to the heart and brain. In some cases, doctors may also use amiodarone or lidocaine for abnormal heart rhythms.
High-quality CPR is the most important step because it keeps blood and oxygen moving. You should push fast, push deep, and avoid long pauses.
