
American Heart Association Training Center
Pediatric tachyarrhythmia with a pulse is a condition where a child’s heart beats much faster than normal while still maintaining a detectable pulse. It can happen suddenly or develop over time and may cause symptoms such as palpitations, dizziness, shortness of breath, or fainting. This fast heartbeat can result from various causes, including heart problems, infections, or imbalances in electrolytes. Because the underlying reasons can differ, it is important to quickly recognize and manage the situation to prevent complications and keep the child safe.
The pediatric tachyarrhythmia with a pulse algorithm is a structured guide that helps healthcare providers decide the best steps to take based on the child’s heart rate, stability, and symptoms. It helps clinicians quickly assess whether the child is stable or unstable, choose the right treatments, and determine if urgent interventions like medications or procedures are needed. By following this approach, doctors can act confidently, reduce risks, and improve outcomes while making the process clear and systematic even in stressful situations.
Note: This pediatric tachyarrhythmia with a pulse algorithm guideline is valid for 2025–2030

Curious about how a child’s normal heart rate compares to the faster heartbeat seen in tachycardia? Let’s explore what these differences mean for kids’ health and well-being.
Age Group | Normal Heart Rate (bpm) | Tachycardia (bpm) |
Infants (1-12 Months) | 80-160 bpm | 160+ bpm |
Toddlers (1-2 Years) | 80-130 bpm | 130+ bpm |
Preschool (3-5 Years) | 80-120 bpm | 120+ bpm |
School Age ( 6-11+ Years) | 70-120 bpm | 120+ bpm |
Managing a fast heart rate in children can feel scary, but clear steps make it easier. This guide walks you through how to check, treat, and keep the child safe.
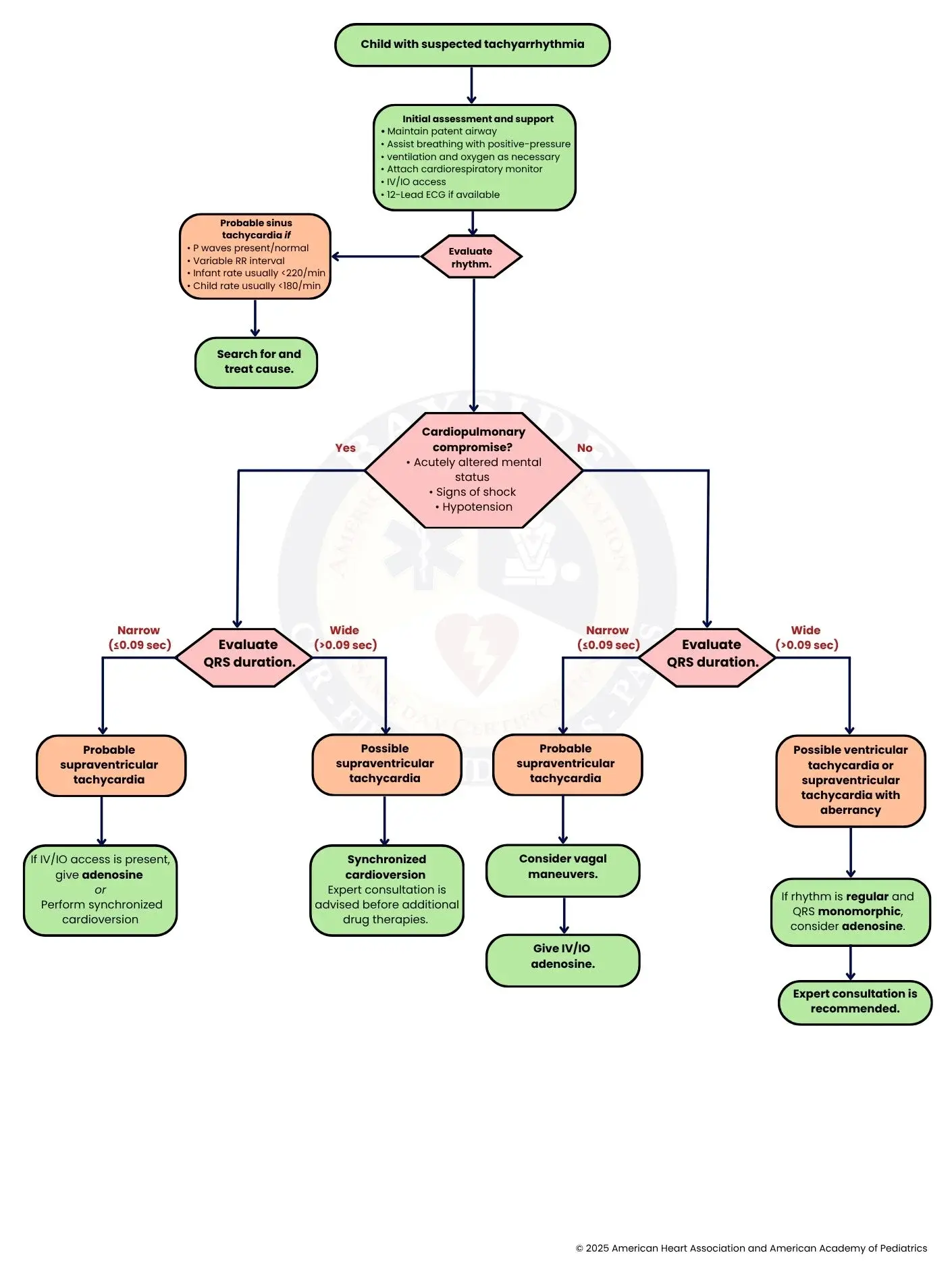
The first step is identifying a child who may have tachyarrhythmia. This is usually suspected when the child presents with a rapid heart rate that is unusually high for their age, or when there are associated symptoms such as palpitations, dizziness, syncope, or signs of poor perfusion. Recognition at this stage is crucial for prompt management.
Immediate stabilization is key. Ensure the airway is patent and provide assisted ventilation with oxygen if needed. Attach a cardiorespiratory monitor to track heart rate, rhythm, and oxygen saturation. Establish intravenous (IV) or intraosseous (IO) access for fluid and medication administration. If possible, obtain a 12-lead ECG (Electrocardiogram) to guide rhythm diagnosis. Proceed to Step 3.
After stabilization, determine the type of tachyarrhythmia. Assess the rhythm from the monitor or ECG. If it appears to be sinus tachycardia (ST), proceed to Step 4. If there are signs of cardiopulmonary compromise, such as shock or altered mental status, proceed to Step 6.
Sinus tachycardia is often physiologic and secondary to fever, pain, dehydration, or anxiety. Signs include visible P waves before each QRS, a variable RR interval, and rates typically less than 220 bpm in infants and less than 180 bpm in older children. Proceed to Step 5.
Address the underlying trigger rather than the heart rate itself. This may involve treating infection, correcting hypovolemia, relieving pain, managing anxiety, or discontinuing stimulants. Successful treatment of the cause usually resolves the tachycardia.
Determine if the child is unstable. Signs include acutely altered mental status, hypotension, poor perfusion, or signs of shock. If these are present, proceed to Step 7. If the child is stable, proceed to Step 12.
Measure the width of the QRS complex. A narrow QRS (≤0.09 seconds) suggests a supraventricular origin, while a wide QRS (>0.09 seconds) may indicate ventricular tachycardia or supraventricular tachycardia (SVT) with aberrant conduction. If narrow, proceed to Step 8. If wide, proceed to Step 10.
A narrow QRS with tachycardia usually indicates SVT. This rhythm often presents as regular and very rapid. Proceed to Step 9.
If IV/IO access is available, adenosine can be administered to terminate the arrhythmia. If not, or if the child is critically unstable, perform synchronized cardioversion. The goal is rapid restoration of normal rhythm while maintaining perfusion.
A wide QRS rhythm in an unstable child raises concern for VT. Immediate management is crucial due to the risk of sudden cardiac arrest. Proceed to Step 11.
Deliver synchronized cardioversion promptly to restore normal rhythm. Consultation with a pediatric cardiologist or arrhythmia specialist is recommended before additional drug therapy, as these rhythms can be life-threatening.
For a stable child, reassess QRS width. A narrow QRS suggests SVT; proceed to Step 13. Wide QRS suggests VT or SVT with aberrancy; proceed to Step 16.
A stable child with narrow QRS tachycardia likely has SVT. Management at this stage focuses on non-pharmacologic interventions first. Proceed to Step 14.
Vagal maneuvers, such as ice to the face or the Valsalva maneuver, can terminate SVT in stable patients by stimulating the parasympathetic nervous system. Proceed to Step 15.
If vagal maneuvers fail, administer adenosine via IV/IO access. Adenosine transiently blocks AV node conduction, often terminating SVT and confirming the diagnosis.
Wide QRS tachycardia in a stable child may be VT or SVT with abnormal conduction. Careful evaluation and preparation for potential escalation are needed. Proceed to Step 17.
If the rhythm is regular and QRS complexes are monomorphic, adenosine may be attempted under careful monitoring. Proceed to Step 18.
Consult a pediatric cardiologist or arrhythmia specialist for guidance on further management, additional drug therapy, and long-term planning. This ensures safe and effective treatment for complex or refractory tachyarrhythmias.
In SVT, the normal electrical activity of the heart is disrupted, so the P waves (which represent atrial contraction) may not be visible or may look unusual on the ECG. This happens because the rapid rhythm often originates above the ventricles and overrides normal sinus node activity.
The RR interval (time between heartbeats) is usually very regular in SVT. Unlike some other arrhythmias where the rhythm varies, SVT produces a steady, fixed rate without noticeable variation between beats.
In infants, SVT typically presents with a very fast heart rate, equal to or greater than 220 beats per minute. This is significantly higher than normal infant heart rates and is a key diagnostic clue.
In older children, SVT is suspected when the heart rate is 180 beats per minute or higher. While children can normally have faster heart rates than adults, rates at or above this level are concerning for abnormal tachyarrhythmia.
SVT often starts and stops suddenly. A history where the child’s heart rate rapidly switches from normal to very fast (and sometimes back to normal just as quickly) strongly suggests SVT rather than gradual causes like fever or dehydration.
This is used when the child is unstable. The initial energy dose is 0.5-1 Joule per kilogram. If the first attempt fails, it is increased to 2 Joules per kilogram. Sedation can be given if the child is conscious, but treatment should not be delayed in emergencies.
Adenosine is the first-line medication for stable SVT. The initial dose is 0.1 mg/kg (maximum 6 mg), given as a rapid IV or IO push, followed immediately by a saline flush to ensure the drug reaches the heart quickly.
If the first dose is ineffective, a second dose of 0.2 mg/kg can be given (maximum 12 mg), again as a rapid push followed by a flush. This higher dose increases the chance of interrupting the abnormal rhythm and restoring the normal sinus rhythm.
In summary, pediatric tachyarrhythmia with a pulse can look alarming, but a clear and steady approach makes a big difference. By checking the child’s condition, understanding the heart rhythm, and acting step by step, healthcare providers can respond quickly and safely. Focusing on the child’s symptoms and overall stability helps guide the right treatment, whether that means fixing an underlying cause or giving urgent care. This structured method brings confidence during stressful moments and supports better outcomes.
With the right knowledge and calm action, it becomes much easier to protect the child and restore a healthy heart rhythm. Ready to improve your skills and respond with confidence? Enroll in a PALS course with Bayside CPR today.
It means a child’s heart is beating much faster than normal, but you can still feel a pulse. This can cause symptoms like dizziness, fast pounding in the chest, or trouble breathing.
Quick recognition helps doctors act fast and prevent serious problems. It also keeps the child safe by starting the right treatment early.
Doctors look for warning signs like low blood pressure, confusion, or poor blood flow. If these signs are present, the child is unstable and needs urgent care.
The first step is to check the child’s airway, breathing, and circulation. Doctors also connect monitors and give oxygen or fluids right away.
If the child is stable, doctors try simple actions like vagal maneuvers to slow the heart. If that doesn’t work, they can give a medicine called adenosine to restore a normal rhythm.
