
American Heart Association Training Center
In a cardiac emergency, a structured, evidence-based approach is essential for improving patient survival and neurological outcomes. The ACLS Algorithm (Advanced Cardiovascular Life Support algorithm) provides a standardized clinical framework used by healthcare professionals to manage life-threatening cardiovascular conditions such as cardiac arrest, bradycardia, and tachycardia.
The American Heart Association (AHA) updates its CPR and ECC Guidelines periodically based on emerging clinical evidence and resuscitation research. The most recent ACLS algorithm updates emphasize key components of high-quality resuscitation care, including effective chest compressions, early defibrillation, advanced airway management, optimized vasopressor and antiarrhythmic drug administration, and structured post–cardiac arrest care.
These algorithms are structured as step-by-step clinical decision pathways rather than simple flowcharts. They are grounded in extensive research, randomized controlled trials, and real-world clinical data, all aimed at improving return of spontaneous circulation (ROSC), survival to discharge, and long-term neurological outcomes.

The ACLS algorithm is vital in emergencies, providing a structured, evidence-based approach to life-threatening cardiovascular events. Its importance includes:
In short, ACLS algorithms are important because they save lives, standardize care, reduce errors, and provide a clear, evidence-based roadmap for handling the most critical cardiovascular emergencies.
The 2025 AHA ACLS updates bring important changes that guide how teams respond during cardiac emergencies. These updates focus on clearer priorities, stronger evidence, and simpler decisions to improve patient outcomes.
NEW Clear Recommendation (2025):
i. IV access is RECOMMENDED as the first choice for drug administration in cardiac arrest.
ii. IO (intraosseous) access is REASONABLE if initial IV attempts are unsuccessful or not feasible.
Why It Matters: A 2025 ILCOR systematic review, including three recent large randomized controlled trials, found that IO access compared with IV access was associated with lower rates of achieving sustained ROSC. While IO remains a valuable rescue option when IV access cannot be established, the evidence now supports prioritizing IV access when possible.
Clinical Impact: EMS systems and hospital code teams should emphasize IV access skills and consider IO as backup rather than an equal first choice.
UPDATED Recommendation (2025): For patients in cardiac arrest with a shockable rhythm, it is reasonable to administer epinephrine AFTER initial defibrillation attempts have failed.
Why It Matters: The evidence supports prioritizing rapid defibrillation over medication administration for shockable rhythms. Epinephrine should be administered after CPR and defibrillation are unsuccessful, not as a first-line intervention alongside initial shocks.
Timeline: This typically means giving epinephrine after 2-3 failed defibrillation attempts while continuing high-quality CPR.
UPDATED (2025): Vasopressin alone or vasopressin in combination with epinephrine offers NO advantage as a substitute for epinephrine in cardiac arrest.
Why It Matters: Multiple systematic reviews and meta-analyses have consistently found no difference in survival outcomes when comparing vasopressin (alone or combined) versus epinephrine alone. This settles a long-standing question in resuscitation medicine.
Clinical Impact: Stop stocking and using vasopressin for cardiac arrest – epinephrine is the sole recommended vasopressor.
NEW (2025):
i. Vector Change Defibrillation: Usefulness “not well established” for refractory VF/pVT
ii. Double Sequential Defibrillation: Usefulness “not well established” for refractory VF/pVT
Why It Matters: Despite industry interest and theoretical benefits, current evidence from clinical trials is insufficient to recommend either vector change or double sequential defibrillation as routine strategies. A single small RCT supports their use, but numerous questions remain about timing, pad placement, and patient selection.
Clinical Guidance: Continue standard defibrillation protocols; these alternative strategies remain investigational.
UPDATED (2025):
i. Atrial Fibrillation: Initial energy setting of ≥200J is reasonable (increased from previous recommendations).
ii. Atrial Flutter: 200J may be reasonable for initial cardioversion.
Why It Matters: Recent randomized trials involving over 3,000 patients with atrial fibrillation found that 200J shocks achieved >90% cumulative cardioversion success across all three currently available US biphasic defibrillator platforms. Lower energy settings were associated with higher failure rates and the need for repeat shocks.
Additionally, low-energy monophasic shocks were more likely to provoke ventricular fibrillation when cardioverting AF compared to higher-energy (≥200J) biphasic shocks.
Clinical Impact: Start with 200J for AF/flutter cardioversion rather than traditional lower energy levels.
NEW (2025): Head-up CPR is NOT recommended except in the setting of clinical trials.
Why It Matters: A recent ILCOR systematic review found no RCTs and only 3 observational studies with significant methodological limitations. The evidence certainty is “very low” for any benefit on survival or a favorable neurologic outcome.
Clinical Guidance: Despite device availability and marketing, head-up CPR should not be implemented outside research protocols.
NEW (2025): For adults in cardiac arrest, the use of β-blockers, bretylium, procainamide, or sotalol for VF/pVT unresponsive to defibrillation is of uncertain benefit.
Why It Matters: No new evidence supports these alternative antiarrhythmic agents. Amiodarone and lidocaine remain the recommended antiarrhythmic options during cardiac arrest.
Note: Bretylium tosylate was recently reintroduced to the US market, but no new evidence supports its effectiveness or safety compared to current recommendations.
UPDATED (2025): Hypotension should be avoided after ROSC by maintaining a minimum MAP of at least 65 mmHg.
Why It Matters: Four randomized trials compared lower versus higher MAP targets after OHCA and found no benefit from targeting higher MAP (e.g., 80-100 mmHg). A minimum MAP of 65 mmHg represents an appropriate balance between avoiding hypotension and preventing potential harms of excessive vasopressor use.
Information Source: Project Heartbeat
The main cardiac arrest algorithm forms the backbone of ACLS, while several specialized sub-algorithms guide providers through specific clinical scenarios. Each sub-algorithm addresses a particular situation and follows its own step-by-step decision pathway.
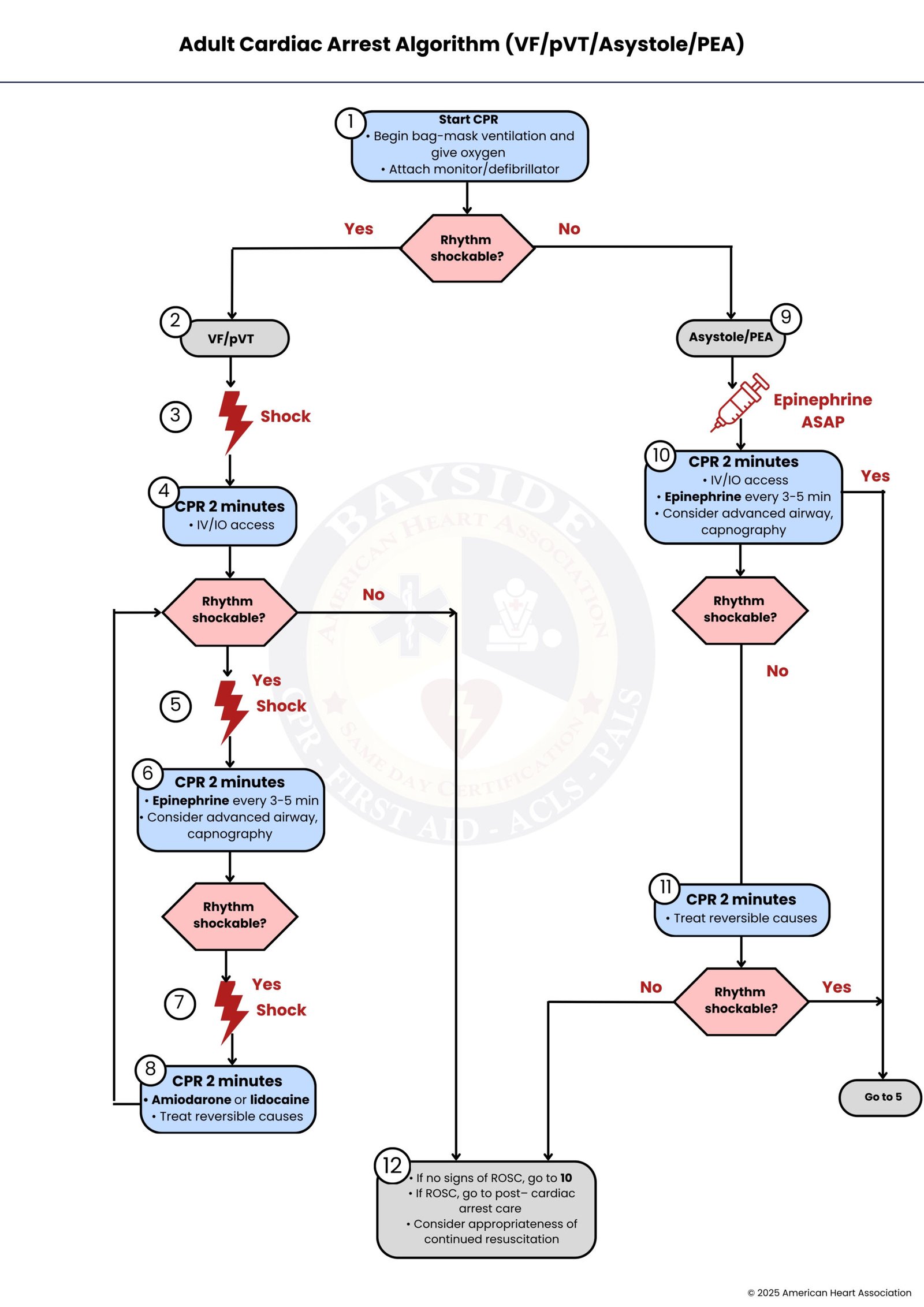
Guides rapid assessment of cardiac arrest, distinguishing shockable (VF/pVT) from non-shockable rhythms (asystole/PEA). Key steps: high-quality CPR, rapid defibrillation, timely epinephrine/antiarrhythmics, airway management, and identifying reversible causes (Hs & Ts) to maximize ROSC and survival.
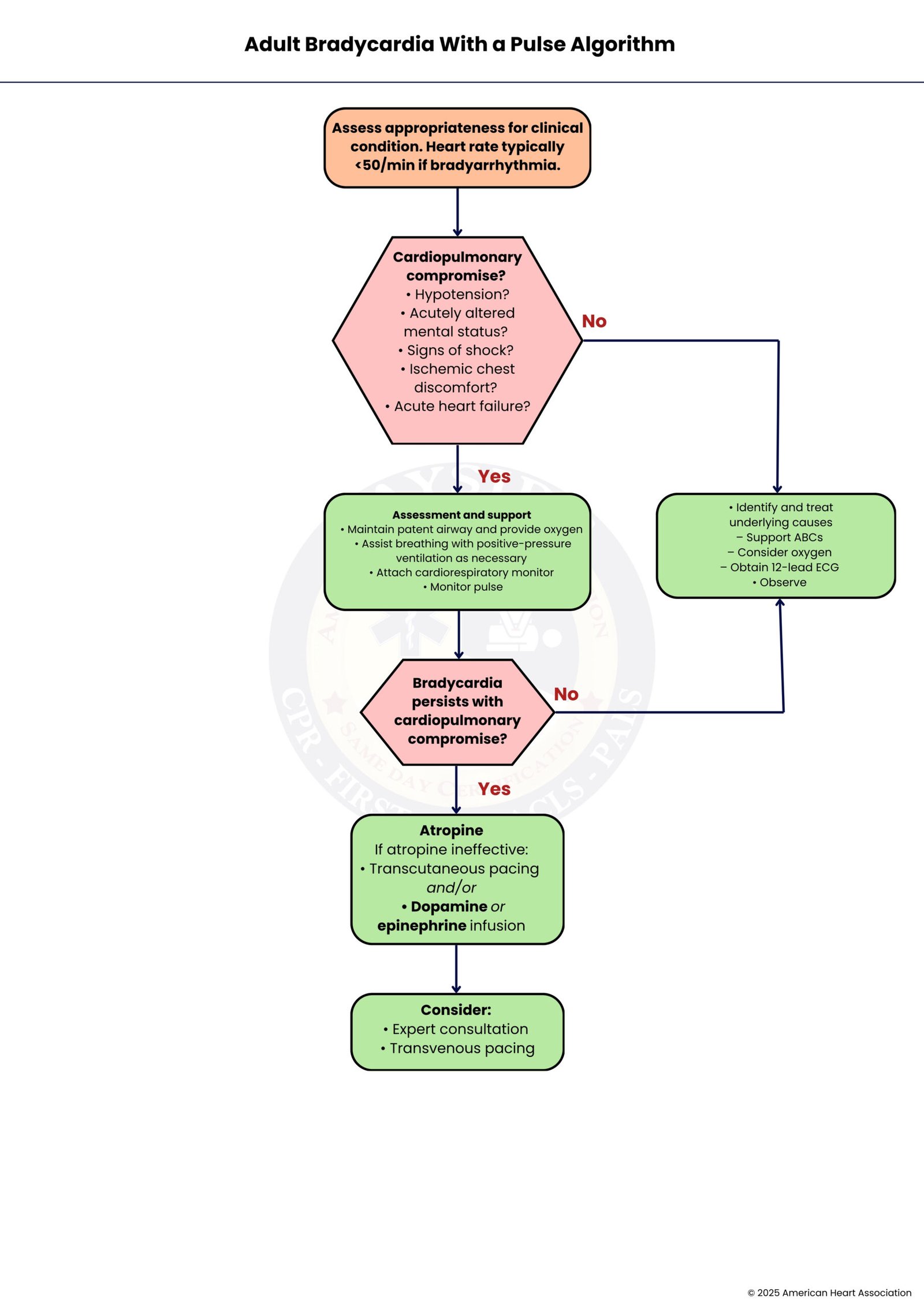
Manages adults with a heart rate <60 bpm with a pulse. Assess stability, vital signs, and reversible causes. Symptomatic patients: oxygen, atropine, pacing, dopamine/epinephrine infusion. Stable patients: monitoring and supportive care. Ensures perfusion and reduces the risk of complications.
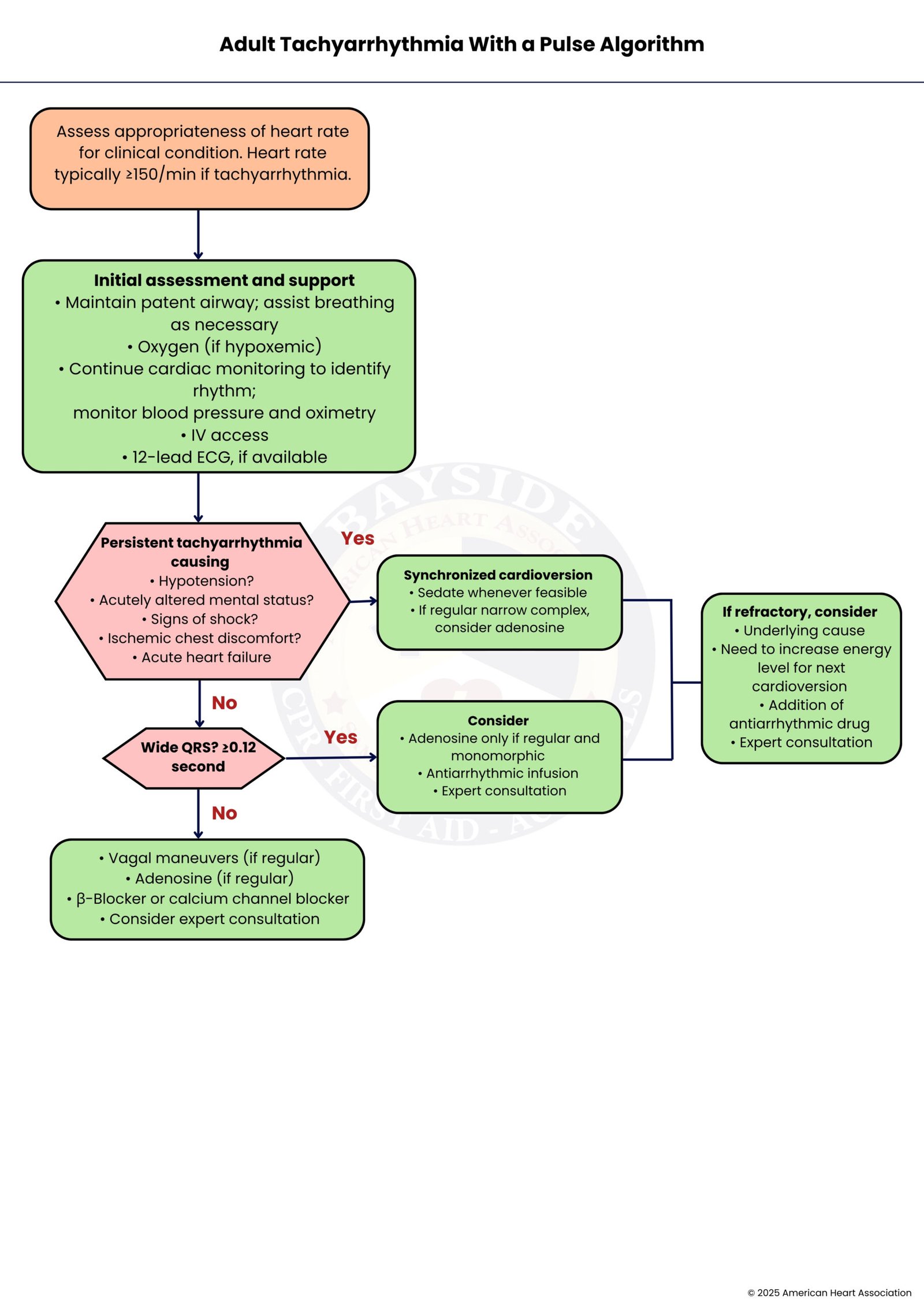
Manages adults with rapid heart rate and pulse. Assess stability, classify rhythm via ECG (narrow vs wide complex). Stable patients: vagal maneuvers, medications, expert consultation. Unstable patients: urgent synchronized cardioversion ± antiarrhythmics. Goal: prevent progression to cardiac arrest and guide therapy.
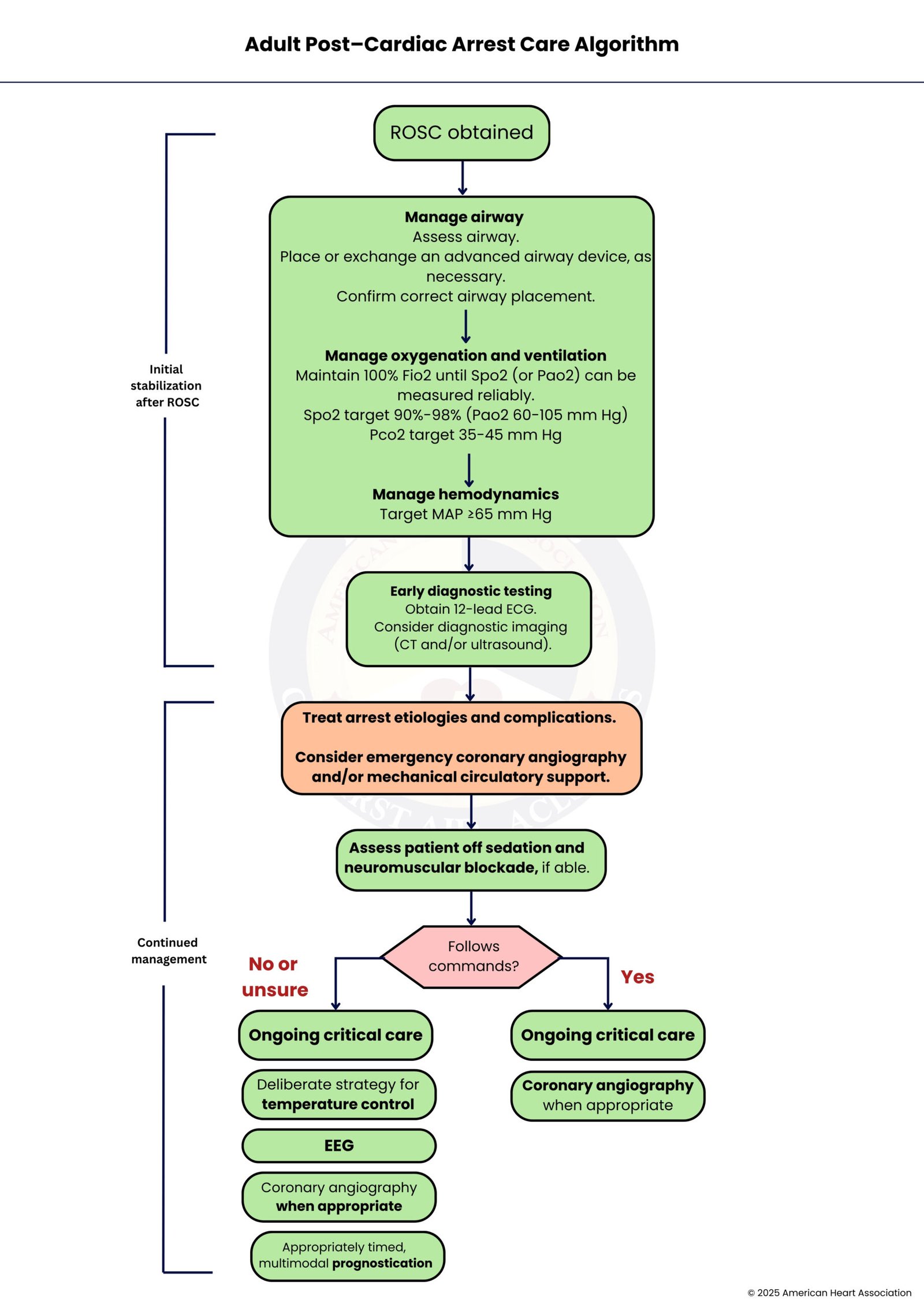
Focuses on stabilizing patients after ROSC. Key steps: optimize oxygenation/ventilation, maintain blood pressure, temperature control, assess neurological status, perform early diagnostics, manage complications, and consider coronary interventions. Goal: improve organ recovery, prognosis, and survival.
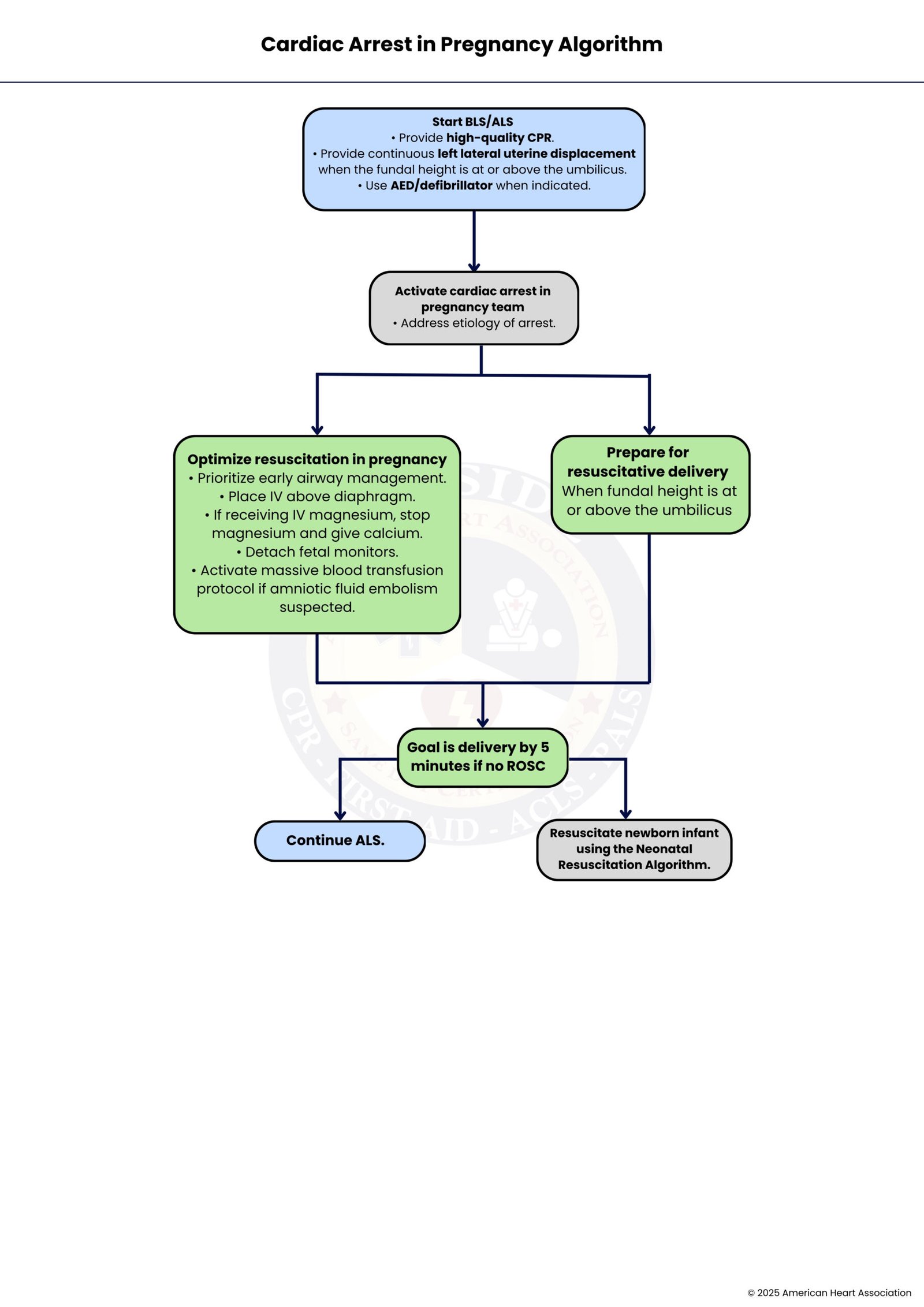
ACLS with pregnancy-specific modifications. High-quality CPR with left uterine displacement, airway management, treating reversible causes, and activating the multidisciplinary team. ≥20 weeks of gestation: perimortem cesarean if no ROSC within 4–5 minutes. Ensures maternal resuscitation and fetal/neonatal care for optimal survival.
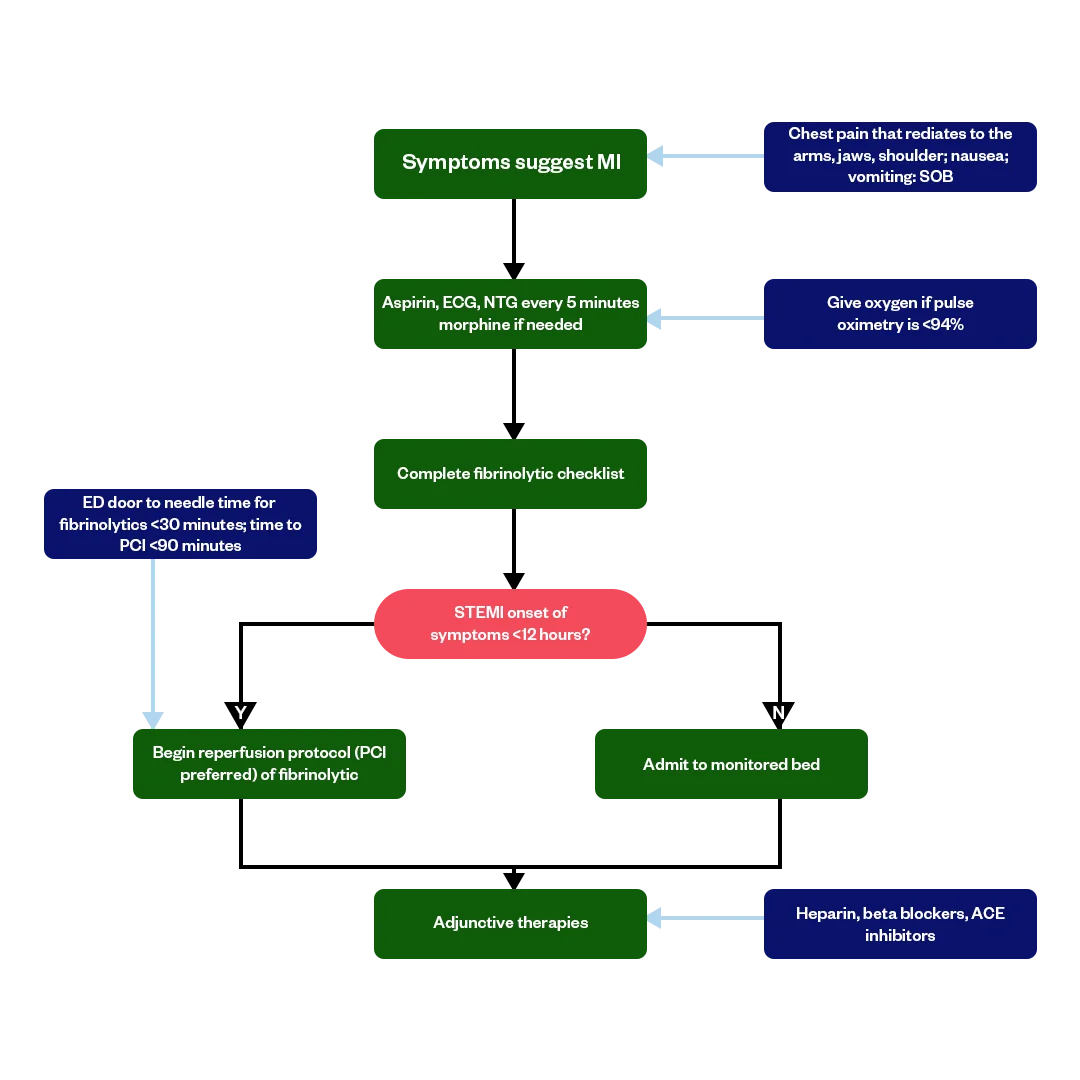
Rapid identification of ACS through ECG and biomarker testing is key. Immediate interventions include aspirin, nitroglycerin, oxygen (if hypoxic), and consideration for reperfusion therapy.
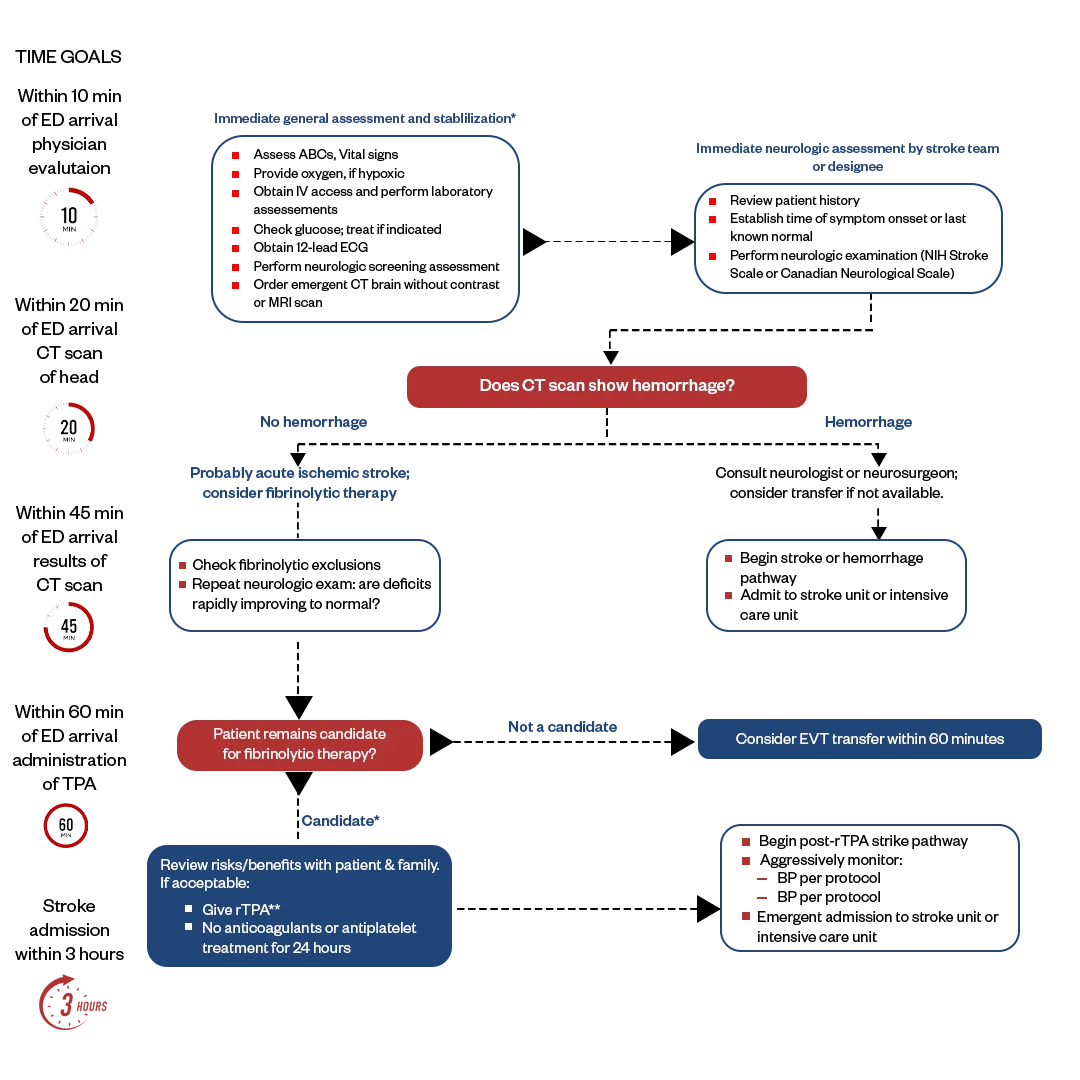
Early recognition and intervention are crucial. The algorithm emphasizes the FAST assessment (Face drooping, Arm weakness, Speech difficulty, Time to call 911) and rapid transport to a stroke-ready hospital.
“Note: AHA hasn’t updated the Acute Coronary Syndrome (ACS) and Suspected Stroke Algorithm in 2025, so they still follow the 2020 guidelines.”
Cardiac arrest can happen because of several underlying problems in the body that can sometimes be reversed if found quickly. Knowing Hs & Ts helps you think fast and treat the real issue instead of only responding to the symptoms.
Always assess and treat these causes systematically during ACLS interventions to maximize survival outcomes.
ACLS courses are for healthcare professionals who are involved in emergency cardiovascular care, including:
Even experienced providers benefit from ACLS training, as updates to algorithms occur regularly based on the latest research.
The ACLS algorithm is more than a protocol. It gives structure to a chaotic emergency and helps teams deliver a coordinated, evidence-based response. Every step, from the first compression to post-resuscitation care, improves survival because research supports it.
Four core actions drive outcomes: high-quality CPR, rapid defibrillation for shockable rhythms, timely epinephrine, and active identification of reversible causes using the H’s and T’s. These pillars determine whether a patient survives with good neurological function.
ACLS is not something you learn once and forget. It is a skill that fades without practice. Providers perform best during real cardiac arrests when they have trained repeatedly and know the algorithm so well that their actions become automatic under pressure.
Enroll in the ACLS course today at Bayside CPR. Start online at your convenience, then complete a quick hands-on skills session in person. Become fully AHA-certified and ready to act when it matters most.
The ACLS algorithm is a step-by-step emergency protocol that healthcare providers use during life-threatening cardiac events. It guides the sequence of CPR, defibrillation, medication use, and post-resuscitation care to improve survival.
Start immediately if the patient is unresponsive, not breathing normally, or has no pulse. Confirm this within 10 seconds. Do not wait for more assessment. Activate the emergency response system, begin CPR, and follow the algorithm right away.
The H’s and T’s help providers remember the most common reversible causes of cardiac arrest. The H’s include hypovolemia, hypoxia, acidosis, electrolyte imbalances, and hypothermia. The T’s include tension pneumothorax, cardiac tamponade, toxins, and coronary or pulmonary thrombosis. Identifying and treating these causes during resuscitation is essential for survival.
Use defibrillation for shockable rhythms such as ventricular fibrillation and pulseless ventricular tachycardia. Deliver the shock as early as possible and resume CPR immediately. Do not use defibrillation for non-shockable rhythms, such as asystole or PEA. Focus on CPR and treating reversible causes instead.
Begin post-resuscitation care immediately. Stabilize blood pressure and oxygenation, obtain a 12-lead ECG to check for STEMI, start targeted temperature management when appropriate, and transfer the patient to the ICU. The goal is to prevent another arrest and protect brain function.