
When someone experience sudden cardiac arrest(SCA), doctors and paramedics need to find and fix the reason it happened as fast as possible. To remember the main reasons, they use a simple list from Advanced Cardiac Life Support (ACLS) called the Hs and Ts(often referred to as H’s and T’s or simply H and T).Think of it like a mechanic’s checklist for a car that won’t start. Instead of just trying to start it over and over (like doing chest compressions), they quickly check: Is there gas? Is the battery dead?The Hs and Ts are that checklist for the human body during a cardiac arrest. They represent problems that, if identified and treated, can restart the heart.
These causes are categorized into two groups:
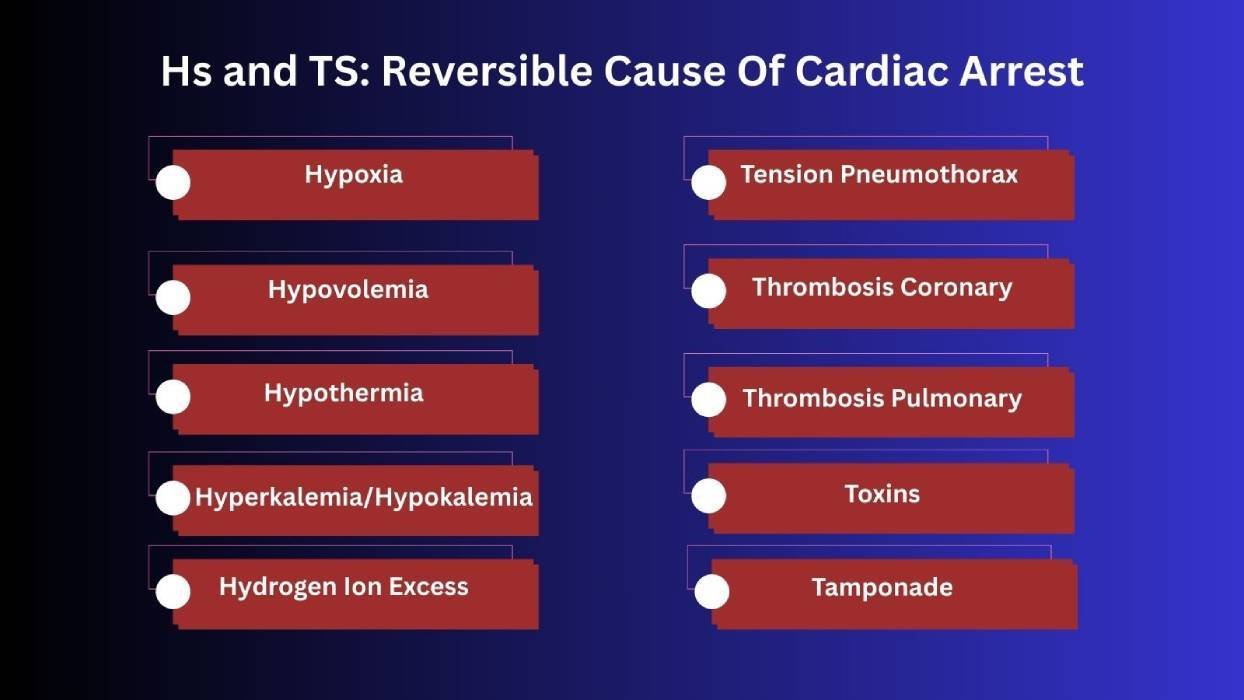
The 5 Hs: These are primarily metabolic or chemical imbalances inside the body (what’s missing or out of balance).
The 5 Ts: These are mostly mechanical or physical problems that block or compress the heart.
By running through this list, you can find the specific cause(a major bleed, a blocked artery, or a drug overdose) and treat it right away while they are doing CPR. This systematic approach is their best chance to save a life.
5 H’s: Reversible Causes of Cardiac Arrest
In emergency situations, identifying and managing issues quickly can make the difference between life and death. The ACLS algorithm emphasizes that while you perform high-quality CPR and defibrillation, you must also systematically search for and treat these underlying “H” causes. They include critical issues like low oxygen, blood loss, or chemical imbalances. Let’s break down each one so you know how to recognize and respond to them.
| H (Cause) | What It Is | Common Causes | Key Symptoms/Signs | Immediate Treatment Goal |
| Hypovolemia (Low Blood Volume) | Severe loss of blood or body fluids. | Trauma, severe bleeding, dehydration, burns. | Fast heart rate, weak pulse, low blood pressure, pale skin. | Replace fluids fast and stop any bleeding. |
| Hypoxia (Lack of Oxygen) | The body or brain is not getting enough oxygen. | Choking, lung failure, low-oxygen environments. | Blue lips/skin, low oxygen reading, confusion, no chest movement. | Ensuring adequate ventilation and maximum oxygen delivery with advanced airway management. |
| Hydrogen Ion Excess (Acidosis) | Too much acid in the blood. | Severe infection (sepsis), kidney failure, lung failure. | Deep/fast breathing, low blood pH, ECG changes, unresponsiveness. | Improving blood flow with CPR; sometimes specific medications to correct respiratory acidosis or metabolic causes. |
| Hyperkalemia (High Potassium) or Hypokalemia (Low Potassium) | Hyperkalemia: Dangerous high level of potassium in the blood. Hypokalemia: Dangerous low level of potassium in the blood. | Hyperkalemia: Kidney failure, some medications, severe tissue injury. Hypokalemia: Diuretics(“water pills”), vomiting, diarrhea, poor diet. | Hyperkalemia: ECG: Peaked T-waves, wide QRS. Muscle weakness, arrhythmias. Hypokalemia: ECG: Flattened T-waves, U-waves. Muscle Cramp, weakness, arrhythmias. | Hyperkalemia: Protect the heart with calcium; shift potassium into cells with insulin/glucose. Hypokalemia: Carefully replace potassium via IV or by mouth. |
| Hypothermia (Low Body Temp) | The body’s core temperature drops dangerously low. | Cold exposure, near-drowning, trauma in cold settings. | Core temp < 35°C (95°F), cold skin, slow heart rate, unconsciousness. | Warm the patient gently with blankets, warm IV fluids, and heated oxygen. |
5 T’s: Reversible Causes of Cardiac Arrest
The T reversible causes of reversible cardiac arrest focus on physical problems that block or disrupt the heart’s function. These include trauma, pressure buildup, and clots. Here’s a breakdown to help you recognize and respond to each one:
| T (Cause) | What It Is | Why It Stops the Heart | Key Symptoms/Signs | Immediate Treatment Goal |
| Tension Pneumothorax | Air trapped in the chest, squeezing the heart and lung. | Chest trauma, lung injury, ventilator complication. | Sudden shortness of breath, uneven chest movement, no breath sounds on one side, distended neck veins. | Relieve pressure instantly with needle decompression, then insert a chest tube. |
| Tamponade (Cardiac) | Fluid or blood filling the sac around the heart, squeezing it. | Chest trauma, cancer, infection (pericarditis). | Muffled heart sounds, distended neck veins, low blood pressure that drops when breathing in. | Drain the fluid immediately with a needle (pericardiocentesis). |
| Toxins | Poisoning or drug overdose disrupting heart rhythm and function. | Overdose of prescription meds (e.g., beta-blockers), recreational drugs (e.g., opioids, cocaine), chemical poisoning. | Abnormal ECG, altered pupils, seizures, confusion, coma. | Provide supportive care, use specific antidotes, and contact poison control. |
| Thrombosis – Coronary (Heart Attack) | A clot blocking a heart artery, stopping blood flow to heart muscle. | Coronary artery disease, blood clot formation. | Chest pain before arrest, ECG shows ST elevation, elevated cardiac enzymes. | Open the blocked artery with angioplasty (PCI) or clot-busting drugs (if done early, before arrest). |
| Thrombosis – Pulmonary (Pulmonary Embolism) | A clot traveling to and blocking the lung’s main artery. | Blood clot from deep vein thrombosis (DVT) traveling to the lungs. | Sudden collapse, rapid heart rate, history of DVT or recent surgery/sickness. | Administer clot-busting drugs (fibrinolytics) during CPR; consider surgical clot removal. |
Integrating Hs & Ts in Real-Time
Knowing the list is only the beginning. The real skill is using it under pressure. A resuscitation algorithm is your step-by-step guide for doing exactly that. Follow these steps to think like a team leader during a real cardiac arrest.
Step 1: Get the Story in the First 30 Seconds
When you arrive at the scene, your first job in the first thirty seconds is to quickly figure out what caused the emergency before moving on to other checks. Ask bystanders or first responders a few simple questions: what happened right before the event, such as whether the person was choking, which would point to a lack of oxygen, or if there was a car accident that could mean blood loss or heart pressure problems. Also ask if there is any major bleeding or injury, since that directly suggests significant blood loss. Finally, find out if the patient has any known illnesses, like kidney failure, which might mean too much potassium in the blood, or lung disease, which could lead to low oxygen.
Step 2: Assign Your Team to Be Your Eyes and Ears
Effective resuscitation requires parallel processing. You cannot assess everything alone. If you have a team, delegate specific tasks simultaneously: airway management, rhythm monitoring, and vascular access. This structured approach, akin to high-performance team dynamics promoted in ACLS, saves critical minutes.² If you are working alone, you must mentally multitask: while performing compressions, visually scan for major bleeding, ensure the airway is patent, and palpate for uneven chest rise all potential clues to an underlying H or T.
Step 3: Turn the Hs and Ts into “Yes or No” Questions
While high-quality CPR continues, you must integrate ongoing assessment. Systematically convert clinical findings into binary decisions. For example: Is the chest moving unevenly? If yes, act on Tension Pneumothorax. Are the T-waves on the monitor tall and peaked? If yes, act on Hyperkalemia. This rapid, checklist-driven thinking helps narrow the differential diagnosis and is supported by cognitive aids used in emergency medicine to reduce error under stress.
Step 4: Treat What You Find
The entire purpose of the Hs and Ts framework is to trigger specific, time-sensitive treatments. The moment you suspect a cause, you must intervene concurrently with CPR. For instance, needle decompression for a suspected tension pneumothorax or IV calcium and insulin/glucose for hyperkalemia are definitive actions that address the root cause of arrest.⁴ Delaying these treatments until after ROSC (Return of Spontaneous Circulation) is often futile, which is why the ACLS algorithm integrates them into the core CPR cycle.
This is the power of the algorithm. It transforms a panicked situation into a calm, systematic process. You are no longer just doing CPR, you are running a diagnostic hunt, guiding your team to find and fix the reversible cause that could save a life.
Final Thoughts: H’s and T’s of Cardiac Arrest
The Hs and Ts represent a crucial framework for identifying reversible causes of cardiac arrest. By focusing on the above-mentioned specific causes, i.e, 5Hs and 5Ts, healthcare providers assess and treat the underlying conditions. Early recognition and prompt intervention of these reversible causes significantly improve the chances of survival and recovery for patients suffering cardiac arrest. With cardiac arrest, there’s no time to waste.
Build the confidence to act in emergencies with Bayside CPR. Our flexible certification programs are created for busy professionals, letting you complete the online coursework on your own schedule before attending a quick 30-minute, in-person skills session at one of our 60+ locations. You’ll earn your AHA Standard ACLS, BLS, PALS, CPR, or First Aid certification and receive your card the same day.