
American Heart Association Training Center
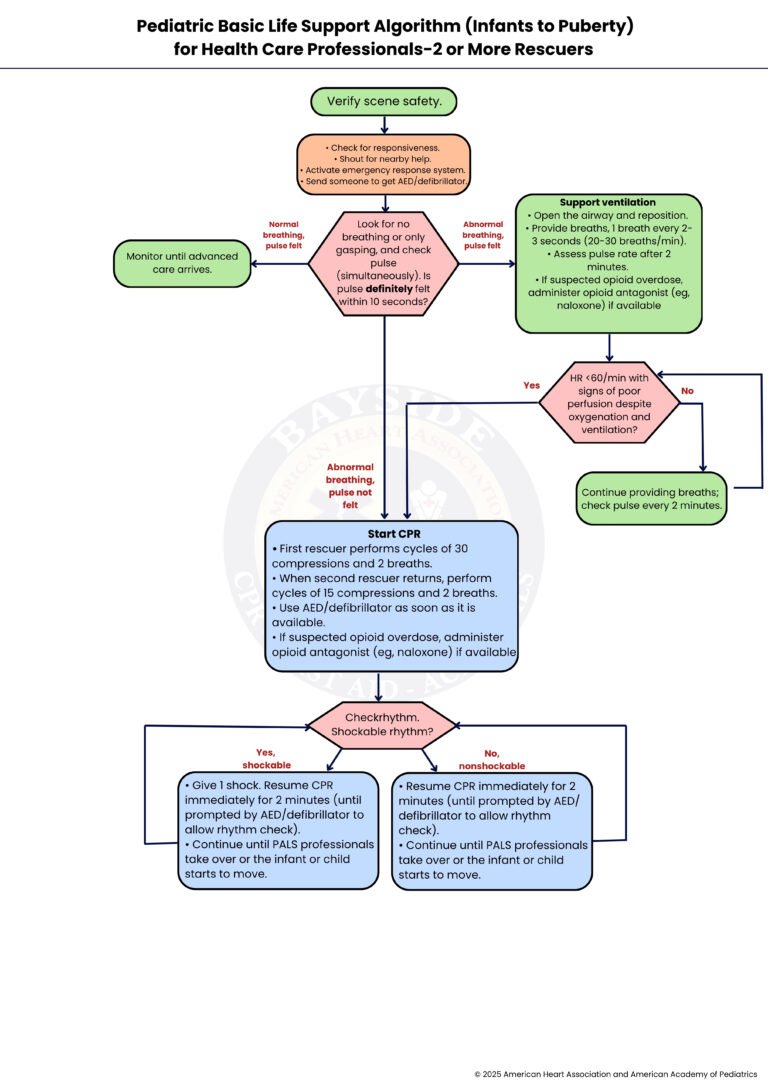
The Pediatric Basic Life Support (BLS) Algorithm for Health Care Professionals—2 or More Rescuers is a step-by-step clinical guideline used during emergencies involving infants and children who are unresponsive, not breathing normally, or have no pulse. It outlines the coordinated actions that trained healthcare providers should follow when at least two rescuers are present. The algorithm includes rapid assessment, activation of emergency response, high-quality chest compressions, ventilation, and early use of an automated external defibrillator (AED) when indicated.
Its main role is to improve survival outcomes in pediatric cardiac arrest or respiratory failure by ensuring a structured, efficient, and team-based response. With multiple rescuers, tasks can be shared, such as one performing compressions while another manages airway and breathing, reducing delays and improving the quality of CPR. This coordinated approach helps maintain oxygen delivery to vital organs and increases the chances of return of spontaneous circulation (ROSC) in children.
Note: This pediatric basic life support algorithm (infants to puberty) for health care professionals—2 or more rescuers guideline is valid for 2025–2030

The Pediatric Basic Life Support recommendations for Healthcare Professionals—2 or More Rescuers represent the official framework published by the American Heart Association for resuscitating infants (under 1 year) and children (from 1 year to puberty). This algorithm is specifically for trained medical teams; it distinguishes itself from the single-rescuer approach by leveraging coordinated teamwork to deliver more efficient and effective care.
The framework presents a sequential flowchart that guides a team of providers through critical decision points. It begins with the simultaneous assessment and activation of the emergency response system by multiple rescuers, then progresses through a coordinated approach to chest compressions, airway management, and the use of an AED.
The 2025 version emphasizes the unique physiology of pediatric patients, where respiratory failure or shock typically precedes cardiac arrest. It streamlines the process by reinforcing the importance of early recognition and rapid support of breathing and circulation, ensuring that the team’s actions are synchronized to minimize interruptions and reduce rescuer fatigue.
We will walk through pediatric basic life support for infants to children up to puberty when two or more rescuers are present. This guide helps you respond quickly and safely during an emergency and support the child with effective care until advanced help arrives.
Verify scene safety by first ensuring that the environment is safe for both the rescuer and the child or infant. Check for any immediate dangers such as traffic, fire, electrical hazards, or unstable surroundings before approaching. Do not proceed with patient contact until the scene is confirmed safe.
Check for responsiveness by gently tapping the infant or child and shouting to assess if there is any reaction. If there is no response, immediately shout for nearby help to alert others. Activate the emergency response system or instruct someone else to do so, and send another person to retrieve an AED/defibrillator without delay to ensure rapid access to advanced care.
Look for no breathing or only gasping and check pulse (simultaneously). This assessment should be completed within 10 seconds by observing chest movement for breathing while palpating the appropriate pulse (brachial for infants, carotid or femoral for children). Is pulse definitely felt within 10 seconds? If there is normal breathing and a pulse is felt, proceed to Step 3a. If there is abnormal breathing but a pulse is felt, proceed to Step 3b. If there is abnormal breathing and a pulse is not felt, proceed to Step 5.
In this situation, the child or infant is breathing adequately and has a detectable pulse, indicating that immediate resuscitation is not required. Continue close monitoring of the patient until advanced care arrives, watching carefully for any deterioration in breathing, responsiveness, or pulse. Be prepared to initiate resuscitation immediately if the condition worsens.
Support ventilation by first opening the airway using appropriate head-tilt–chin-lift or jaw-thrust maneuver if trauma is suspected, and repositioning if necessary. Provide rescue breaths at a rate of 1 breath every 2 to 3 seconds, or approximately 20 to 30 breaths per minute, ensuring visible chest rise. Reassess the pulse after 2 minutes of ventilation. If opioid overdose is suspected and available, administer an opioid antagonist such as naloxone.
Is heart rate less than 60 per minute with signs of poor perfusion despite oxygenation and ventilation? If Yes, this indicates inadequate circulation requiring chest compressions, so proceed to Step 5. If No, the heart rate is adequate, so continue supportive care and move to Step 4a.
Continue providing assisted breaths to maintain adequate oxygenation and ventilation, ensuring effective chest rise with each breath. Reassess the pulse every 2 minutes to monitor for any deterioration in heart rate or perfusion. If the heart rate drops below 60 per minute or becomes absent, promptly return to Step 4 for reassessment and escalation of care.
Start CPR immediately. The first rescuer performs cycles of 30 compressions and 2 breaths if alone, ensuring high-quality compressions with appropriate depth and rate. When a second rescuer becomes available, switch to coordinated cycles of 15 compressions and 2 breaths for better efficiency in pediatric resuscitation. Use the AED/defibrillator as soon as it is available, and follow its prompts. If opioid overdose is suspected, administer an opioid antagonist such as naloxone if available.
Check rhythm using the AED/defibrillator to determine if the cardiac rhythm is shockable. Is it a shockable rhythm?If Yes, it is shockable, proceed to Step 7. If No, it is nonshockable, proceed to Step 8.
Give 1 shock using AED/defibrillator. Immediately resume CPR for 2 minutes without delay, continuing until the AED prompts a rhythm check again or until advanced pediatric life support providers take over. Continue cycles of shock and CPR as indicated.
Resume CPR immediately for 2 minutes, followed by rhythm reassessment using the AED/defibrillator. Continue high-quality CPR cycles and address reversible causes while awaiting or continuing advanced pediatric life support care until the child or infant shows signs of recovery or providers take over.
In short, the pediatric basic life support algorithm for two or more rescuers gives healthcare teams a clear and organized way to respond when an infant or child faces a life-threatening emergency. It guides rescuers to quickly check safety, assess breathing and pulse, and start the right actions without delay. When a team works together, they can share tasks such as chest compressions, breathing support, and equipment use, which helps care stay smooth and fast. This teamwork improves oxygen delivery to vital organs and supports better chances of recovery. By following each step with focus and coordination, rescuers reduce confusion and act more effectively under pressure. The approach also encourages constant reassessment so changes in the child’s condition are noticed early. Overall, this method helps save valuable time and increases the likelihood of a positive outcome in critical situations.
Learning and memorizing these steps equips you to act quickly in an emergency and helps you safeguard others with confidence and care. Enroll in our BLS course at Bayside CPR to gain dependable, life-saving skills for handling adult emergencies.
It is a step-by-step guide for healthcare workers who treat infants and children in emergencies. It helps teams work together to give CPR, support breathing, and use an AED quickly and safely.
Rescuers first check if the scene is safe before touching the child. Then they check responsiveness and call for help while activating emergency services.
They look for normal breathing or gasping and check the pulse within 10 seconds. They use the brachial pulse for infants and the carotid or femoral pulse for children.
With two rescuers, they use 15 chest compressions and 2 breaths. One rescuer does compressions while the other gives breaths to keep CPR high quality.
An AED should be used as soon as it is available in a child’s emergency. It helps check the heart rhythm and tells rescuers if a shock is needed.
